-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2199-2201
doi:10.5923/j.ajmms.20261604.133
Received: Mar. 28, 2026; Accepted: Apr. 20, 2026; Published: Apr. 30, 2026

The Role of Genetic Factors in the Pathogenesis of Juvenile Rheumatoid Arthritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhaldarbekova Malika Akhinjanovna
PhD, Associate Professor, Department of Pediatric Diseases No. 2 Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Khaldarbekova Malika Akhinjanovna, PhD, Associate Professor, Department of Pediatric Diseases No. 2 Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Juvenile rheumatoid arthritis (JRA) is a chronic autoimmune inflammatory disease characterized by persistent joint inflammation and progressive functional impairment in children. Genetic predisposition plays a critical role in the development and progression of the disease; however, the specific mechanisms underlying this association remain incompletely understood. This study aims to investigate the contribution of genetic factors, particularly human leukocyte antigen (HLA) alleles and non-HLA gene polymorphisms, in the pathogenesis of JRA. A comprehensive analysis was conducted involving pediatric patients diagnosed with JRA and a control group of healthy children. Genetic screening included the evaluation of HLA class II alleles, as well as polymorphisms in genes associated with immune regulation, such as PTPN22, STAT4, and TNF-α. Clinical data were correlated with genetic findings to assess their impact on disease severity and progression. The results demonstrated a significant association between specific HLA-DRB1 alleles and increased susceptibility to JRA. Additionally, polymorphisms in immune-related genes were linked to higher disease activity and severity. These findings highlight the importance of genetic predisposition in modulating immune responses and contributing to disease pathogenesis. In conclusion, genetic factors play a pivotal role in the development and clinical course of JRA. Understanding these mechanisms may facilitate early diagnosis, risk stratification, and the development of targeted therapeutic strategies.
Keywords: Juvenile rheumatoid arthritis, Genetics, HLA, Polymorphism, Autoimmune disease, Pediatric rheumatology
Cite this paper: Khaldarbekova Malika Akhinjanovna, The Role of Genetic Factors in the Pathogenesis of Juvenile Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2199-2201. doi: 10.5923/j.ajmms.20261604.133.
1. Introduction
- Juvenile rheumatoid arthritis (JRA), more commonly referred to as juvenile idiopathic arthritis (JIA), is the most prevalent chronic rheumatic disease in children and a leading cause of long-term disability in pediatric populations worldwide. The disease is characterized by persistent synovial inflammation, joint destruction, and systemic manifestations that significantly impair quality of life and functional outcomes [1]. Despite extensive research, the exact etiology of JRA remains multifactorial, involving a complex interplay between genetic susceptibility and environmental triggers. Among these, genetic factors have been identified as key determinants influencing both disease onset and progression. Family-based and twin studies have demonstrated a significantly higher concordance rate among monozygotic twins compared to dizygotic twins, highlighting the strong heritable component of the disease [2]. One of the most extensively studied genetic contributors to JRA is the human leukocyte antigen (HLA) system, particularly class II alleles such as HLA-DRB1 and HLA-DQ. These molecules play a crucial role in antigen presentation and immune response modulation. Specific HLA alleles have been associated with increased susceptibility to certain subtypes of JRA, as well as variations in disease severity and clinical manifestations [3]. In addition to HLA genes, non-HLA genetic polymorphisms have also been implicated in the pathogenesis of JRA. Genes involved in immune regulation, including PTPN22, STAT4, IL2RA, and TNF-α, have been shown to influence T-cell activation, cytokine production, and inflammatory pathways. Variations in these genes may lead to dysregulation of immune tolerance and the development of autoimmune responses targeting synovial tissues [4]. Recent advances in molecular genetics and genome-wide association studies (GWAS) have further expanded our understanding of the genetic architecture of JRA. These studies have identified multiple susceptibility loci that contribute to disease heterogeneity and individual variability in treatment response [5]. Understanding the role of genetic factors in JRA is essential not only for elucidating disease mechanisms but also for improving early diagnosis, predicting disease course, and developing personalized therapeutic strategies. Therefore, this study aims to investigate the contribution of genetic factors to the pathogenesis of juvenile rheumatoid arthritis and to evaluate their clinical significance in pediatric patients.
2. Materials and Methods
- This study was designed as a prospective observational study conducted at the Department of Pediatric Rheumatology of Tashkent State Medical University between 2022 and 2024. The study included a total of 120 children aged 4 to 16 years, of whom 70 patients were diagnosed with juvenile rheumatoid arthritis (JRA) according to the International League of Associations for Rheumatology (ILAR) classification criteria [6], while 50 age- and sex-matched healthy children formed the control group.Study PopulationInclusion criteria for the patient group were: confirmed diagnosis of JRA, disease duration of at least 6 months, and absence of other autoimmune or chronic inflammatory diseases. Exclusion criteria included the presence of severe comorbidities, acute infections at the time of examination, and prior immunosuppressive therapy within the last three months.Clinical AssessmentAll patients underwent comprehensive clinical evaluation, including detailed medical history, physical examination, and assessment of disease activity. Disease severity was evaluated using the Juvenile Arthritis Disease Activity Score (JADAS-27), [7] which incorporates the number of active joints, physician global assessment, parent/patient global assessment, and erythrocyte sedimentation rate (ESR).Genetic AnalysisPeripheral blood samples were collected from all participants for genetic testing. Genomic DNA was extracted using standard phenol-chloroform methods. HLA typing was performed using polymerase chain reaction (PCR) with sequence-specific primers (PCR-SSP) to identify HLA-DRB1 and HLA-DQ alleles. In addition, selected non-HLA gene polymorphisms, including PTPN22 (rs2476601), STAT4 (rs7574865), and TNF-α (−308 G/A), were analyzed using real-time PCR techniques. [8]Laboratory InvestigationsStandard laboratory tests included complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and rheumatoid factor (RF). Anti-cyclic citrullinated peptide (anti-CCP) antibodies were also measured in selected cases.Statistical AnalysisStatistical analysis was performed using SPSS version 26.0. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were presented as percentages. Differences between groups were assessed using Student’s t-test and chi-square test, as appropriate. The association between genetic polymorphisms and disease susceptibility was evaluated using odds ratios (OR) with 95% confidence intervals (CI). A p-value of <0.05 was considered statistically significant.
3. Results and Discussion
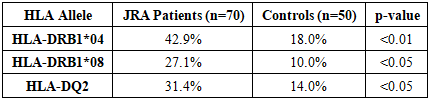
- The analysis of clinical and genetic data revealed significant differences between patients with juvenile rheumatoid arthritis (JRA) and the control group.Among the 70 patients with JRA, the majority were female (62.8%), with a mean age of 10.4 ± 3.2 years. The average disease duration was 2.8 ± 1.1 years. Moderate to high disease activity (JADAS-27 score >10) was observed in 68.5% of patients, indicating a predominantly active disease course. Genetic analysis demonstrated a strong association between specific HLA alleles and susceptibility to JRA. The frequency of the HLA-DRB104 allele was significantly higher in the patient group (42.9%) compared to controls (18.0%) (p<0.01). Similarly, HLA-DRB108 was detected in 27.1% of patients versus 10.0% in controls (p<0.05).
|
4. Conclusions
- This study demonstrates that genetic factors play a fundamental role in the pathogenesis and clinical progression of juvenile rheumatoid arthritis (JRA). The identification of significant associations between specific HLA alleles, particularly HLA-DRB104 and HLA-DRB108, and increased disease susceptibility confirms the importance of antigen presentation mechanisms in the development of autoimmune inflammation. Furthermore, non-HLA gene polymorphisms, including PTPN22 and STAT4, were shown to contribute to immune dysregulation and higher disease activity, highlighting their role in modulating inflammatory pathways. The observed correlation between genetic variants and elevated inflammatory markers emphasizes the clinical relevance of genetic predisposition in determining disease severity. The findings suggest that genetic profiling may serve as a valuable tool for early diagnosis, risk stratification, and prediction of disease course in pediatric patients with JRA. Incorporating genetic markers into clinical practice could facilitate personalized therapeutic approaches and improve long-term outcomes. Despite these promising results, further large-scale, multicenter studies are required to validate these findings and to explore additional genetic loci involved in JRA pathogenesis.In conclusion, a comprehensive understanding of genetic factors is essential for advancing precision medicine in pediatric rheumatology and for developing targeted treatment strategies for juvenile rheumatoid arthritis.