-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2192-2195
doi:10.5923/j.ajmms.20261604.131
Received: Mar. 29, 2026; Accepted: Apr. 21, 2026; Published: Apr. 29, 2026

Prevalence of Chronic Kidney Disease in Patients with Chronic Obstructive Pulmonary Disease and Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYusupova Shaxnoza Kadirjanovna, Delkasheva Shaxloxon Djamolitdinovna, Axmedov Baxtiyor Xabibullayevich, Mirzaaxmedova Irodaxon Zokirjonovna, Yakubbekova Mavludaxon Kozimjonovna
Department of Hospital Therapy and Endocrinology, Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

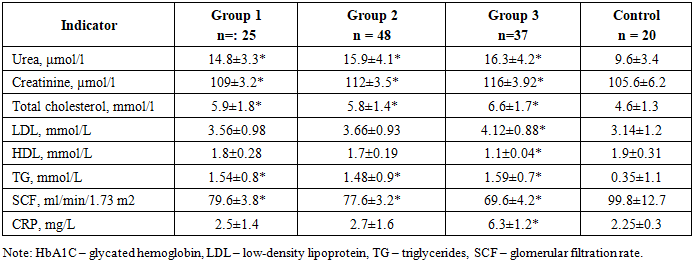
The aim of the study is to assess the prevalence of chronic kidney disease in patients with chronic obstructive pulmonary disease of varying severity and obesity. Material and methods of research. This study included 110 outpatients with a diagnosis of stable COPD who were treated at our clinic from May 2024 to April 2025. For comparison, a control group of 20 age-matched outpatients (60 years and older) without COPD or kidney disease who also visited our hospital during this period was formed. The patients were divided into 3 groups according to severity: Group 1 – patients with mild COPD – 25 people, Group 2 – patients with moderate COPD – 48 people, and Group 3 – patients with severe COPD – 37 patients. Research methods: included general clinical methods (complete blood count, urine analysis), biochemical analyses (blood glucose, bilirubin, both direct and indirect, ALT, AST, PTI, coagulogram, C-reactive protein, urea, creatinine, lipid spectrum, etc.), anthropometric calculations (height (cm), weight (kg), BMI (kg/m2), WC, HC) and instrumental methods: ECG, ultrasound of internal organs, chest X-ray, etc. Research results. When calculating the glomerular filtration rate (GFR) based on creatinine levels, no significant differences were found between groups 1 and 2 (GFR Cr:79.6±3.8against 77.6±3.2ml/min/1.73 m²). At the same time, in patients with severe COPD (group 3), there was a significant decrease in SCF: 69.6±4.2ml/min/1.73 m²). Chronic kidney disease (CKD), defined as a SCF below 60 ml/min/1.73 m², was observed in 15 patients with COPD only in group 3 (15 (40.5%) of 37 in the group or 15 (13.6%) of 110 patients). In patients of group 3, a significant increase in blood creatinine (p<0.005) was found against the background of dyslipidemia (decreased HDL, increased HDL, and the lowest SCF (p< 0.005). In addition, in the groups, the average values of CRP were significantly higher compared to the control group, although in groups 1 and 2 the values were within the normal range. Conclusions. 1. Chronic kidney disease (CKD), defined as an eGFR below 60 ml/min/1.73 m², was observed in 15 patients with COPD in group 3 only (15 (40.5%) of 37 in the group or 15 (13.6%) of 110 patients). 2. Assessing the presence of chronic kidney disease (CKD) in patients with chronic obstructive pulmonary disease (COPD) is of significant clinical value. In particular, CKD is an independent predictor of cardiovascular disease (CVD), which is often comorbid with COPD. Furthermore, identifying CKD may have prognostic value for this patient population.
Keywords: COPD, Obesity, Renal dysfunction
Cite this paper: Yusupova Shaxnoza Kadirjanovna, Delkasheva Shaxloxon Djamolitdinovna, Axmedov Baxtiyor Xabibullayevich, Mirzaaxmedova Irodaxon Zokirjonovna, Yakubbekova Mavludaxon Kozimjonovna, Prevalence of Chronic Kidney Disease in Patients with Chronic Obstructive Pulmonary Disease and Obesity, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2192-2195. doi: 10.5923/j.ajmms.20261604.131.
1. Introduction
- Chronic obstructive pulmonary disease (COPD) is a complex disease affecting the entire body and characterized by systemic inflammation, which leads to the development of various comorbidities. [1-3]. Because these comorbidities significantly impact the severity of COPD and patient prognosis, their active screening and treatment are integral to effective COPD control. [4-6]. Although cardiovascular disease, osteoporosis, and depression are well-known as frequent companions of COPD, the relationship with chronic kidney disease (CKD) remains poorly understood. Furthermore, older age, smoking, and the presence of COPD are themselves risk factors for the development of CKD, which is also a significant risk factor for cardiovascular disease. [7-10]. Recent studies revealing a high frequency of microalbuminuria in patients with COPD have drawn attention to the possible correlation between COPD and CKD. It has been noted that CKD may be missed in elderly patients with COPD and decreased muscle mass if the diagnosis is based solely on creatinine levels. In this regard, cystatin C, [11]. recognized as a biomarker of early renal dysfunction, is of particular importance. A formula for calculating the glomerular filtration rate (eGFR) based on cystatin C levels was developed and proposed, which was adopted by the Japanese Society of Nephrology in 2012, complementing traditional creatinine-based assessment methods [12]. Chronic kidney disease (CKD) and chronic obstructive pulmonary disease (COPD) share common etiopathogenesis, including risk factors such as smoking and age-related changes. It is emphasized that CKD is associated with persistent chronic inflammation. The clinical and prognostic aspects of CKD and COPD also have points of contact, in particular, the significance of cardiovascular diseases as a comorbidity influencing outcome. Despite the insufficient study of CKD in the context of COPD, recent studies indicate a high prevalence of chronic renal failure and microalbuminuria among patients with COPD, which raises the question of the existence of a correlation between these pathologies. [13].Study by Incalzi RA, Corsonello A, Pedone C, et al. [14] indicates the potential presence of latent chronic renal failure (CRF) in a significant proportion of patients with chronic obstructive pulmonary disease (COPD). They note that in such cases, creatinine levels and estimated glomerular filtration rate (eGFR) may remain within the reference range. This phenomenon is explained by a compensatory effect: despite impaired renal excretion of creatinine, reduced muscle mass in patients with COPD leads to a decrease in its endogenous production. The authors also recorded an increased prevalence of CRF in a cohort of elderly patients with COPD (≥ 65 years) compared to a control group of age-matched outpatients. In particular, the combined prevalence of latent and overt CRF in the COPD group was 43%, which was statistically significantly higher than the rate in the control group (23.4%).According to the authors, the differences in COPD prevalence between our study and the work of Incalzi RA, Corsonello A, Pedone C, et al. may be due to the difference in body mass index (BMI). The patients in Incalzi RA, Corsonello A, Pedone C, et al. had a significantly higher mean BMI (27.4 kg/m²) than our patients (21.1 kg/m²). Furthermore, in our non-COPD group, the prevalence of CKD increased from 8% to 15% when using eGFR Cys instead of eGFR Cr. This suggests that the cystatin C (Cys)-based estimation formula may be more accurate for determining decreased kidney function in elderly Japanese patients with low muscle mass. [15].The above formed the basis for this study.Purpose of the study-to assess renal function in patients with chronic obstructive pulmonary disease of varying severity and obesity.
2. Material and Methods of Research
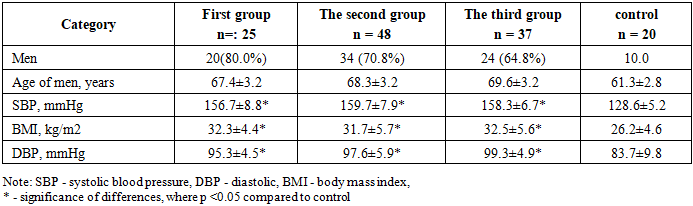
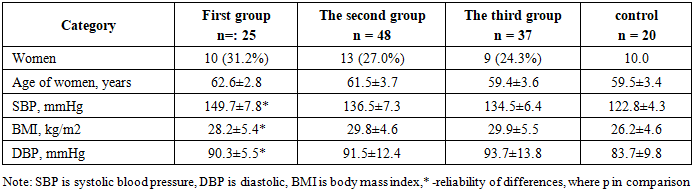
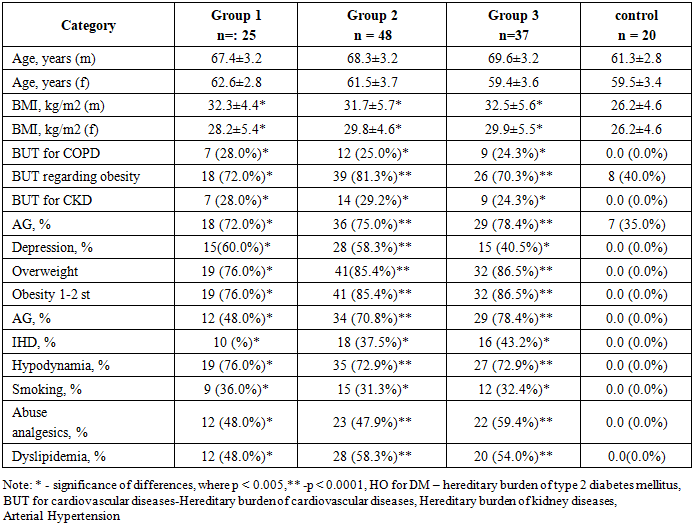
- This study included 110 outpatients with a diagnosis of stable COPD who were treated at our clinic from May 2024 to April 2025. For comparison, a control group of 20 age-matched outpatients (60 years and older) without COPD or kidney disease who also visited our hospital during this period was formed.The study was conducted at Andijan City Clinical Hospital No. 1. There were 78 men and 32 women.The patients were divided into 3 groups according to the severity of COPD: Group 1 – patients with mild COPD – 25 people, Group 2 – patients with moderate COPD – 48 people, and Group 3 – patients with severe COPD – 37 patients.Inclusion criteria: patients with COPD, also suffering from obesity and CKD stages 1-3, men, women, informed written consent.Exclusion criteria: pregnant women, oncology, chronic kidney disease stage 4-5, acute myocardial infarction, stroke, systemic and autoimmune diseases.Research methods: included general clinical methods (complete blood count, urine analysis), biochemical analyses (blood glucose, bilirubin, both direct and indirect, ALT, AST, PTI, coagulogram, C-reactive protein, urea, creatinine, lipid spectrum, etc.), anthropometric calculations (height (cm), weight (kg), BMI (kg/m2), WC, HC) and instrumental methods: ECG, ultrasound of internal organs, chest X-ray, etc.All participants provided written consent to participate in the study. The following parameters were measured: hemoglobin, urea, and creatinine. Chronic kidney disease (CKD) was diagnosed with an estimated glomerular filtration rate (eGFR) below 60 ml/min/1.73 m². The diagnosis of COPD was confirmed by spirometry: the FEV1/FVC ratio was less than 70% after bronchodilator therapy, and the degree of obstruction was assessed using the GOLD classification. Glomerular filtration rate (eGFR) was calculated based on creatinine levels.To compare baseline characteristics of the three groups separated by different degrees of comorbidities, the Kruskal–Wallis test was used for continuous variables and the χ² test for categorical variables.
3. Research Results
- Tables 1 and 2 provide general characteristics of the patients included in the study.
|
|
|
|
4. Conclusions
- 1. Chronic kidney disease (CKD), defined as an eGFR below 60 ml/min/1.73 m², was observed in 15 patients with COPD in group 3 only (15 (40.5%) of 37 in the group or 15 (13.6%) of 110 patients). 2. Assessing the presence of chronic kidney disease (CKD) in patients with chronic obstructive pulmonary disease (COPD) is of significant clinical value. In particular, CKD is an independent predictor of cardiovascular disease (CVD), which is often comorbid with COPD. Furthermore, identifying CKD may have prognostic value for this patient population.