-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2188-2191
doi:10.5923/j.ajmms.20261604.130
Received: Mar. 27, 2026; Accepted: Apr. 20, 2026; Published: Apr. 29, 2026

Integrated Management of Oral Complications in Chronic Diffuse Liver Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKazakova N. N.1, Kurambayeva N. Ya.2
1DSc, Associate Professor, Department of Therapeutic Dentistry, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Dentist, "MEMORIAL HOSPITAL" LLC, Khorezm, Uzbekistan
Correspondence to: Kazakova N. N., DSc, Associate Professor, Department of Therapeutic Dentistry, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

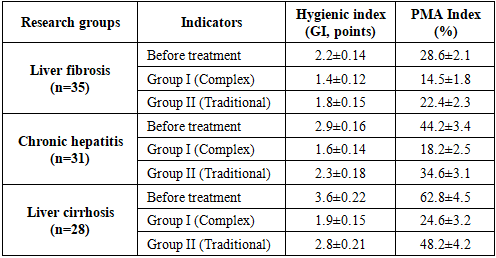
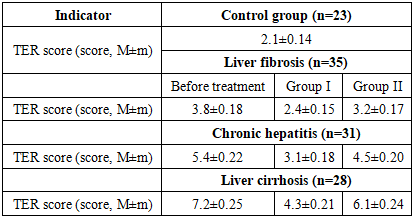
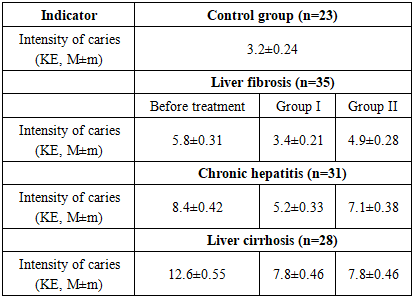
This study focuses on evaluating the dental status of the oral cavity and enhancing treatment outcomes in patients with chronic diffuse liver diseases (CDL). A total of 94 patients participated in the research and were categorized into groups with liver fibrosis, chronic hepatitis, and liver cirrhosis according to the underlying pathology. Two therapeutic strategies were applied: standard dental care and a comprehensive treatment protocol proposed by the author, which included the use of the herbal preparation Rotokan, vitamin C electrophoresis, and UHF (ultra-high-frequency) therapy. The findings demonstrated that the progression of liver disease is associated with worsening dental indices (GI, PMA, KE). In contrast, patients who received the comprehensive treatment exhibited a twofold faster reduction in periodontal inflammation, restoration of enamel resistance, and stabilization of caries progression. Overall, the study provides scientific evidence supporting the high pathogenetic efficacy of an integrated multidisciplinary approach combined with physiotherapeutic modalities in the management of patients with liver-related systemic disorders.
Keywords: Chronic diffuse liver diseases, Liver cirrhosis, Chronic hepatitis, Periodontal disease, Dental caries, Rotokan, Physiotherapy, Dental indices
Cite this paper: Kazakova N. N., Kurambayeva N. Ya., Integrated Management of Oral Complications in Chronic Diffuse Liver Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2188-2191. doi: 10.5923/j.ajmms.20261604.130.
1. Introduction
- Epidemiological data indicate an increase in the number of patients with HDL worldwide, especially as HDL combined with metabolic syndrome has reached the level of a global pandemic. Chronic viral hepatitis is considered one of the most common causes of chronic liver inflammation. According to WHO data, 257 million people worldwide are living with chronic HBV infection. While the probability of chronic HBV infection in adults is less than 5%, in cases of perinatal transmission, this figure reaches 90%. Chronic hepatitis B is a major factor in the development of cirrhosis and HCC [6,7].Chronic diffuse liver diseases (CDL) are a pressing global medical and social problem, the main etiological factors of which are chronic viral hepatitis (B and C), alcoholic liver disease (ALD), and the increasingly widespread fatty liver disease (FLD) associated with metabolic dysfunction. Chronic diffuse liver diseases are characterized by chronic inflammation of the liver parenchyma, necrosis, and progression into liver fibrosis, which ultimately leads to liver cirrhosis and hepatocellular insufficiency [7,10]. The development of the disease is directly linked to the development of severe complications, such as a decrease in the protein-synthetic function of the liver (impaired synthesis of albumin and coagulation factors), impaired detoxification function (accumulation of ammonia), as well as portal hypertension and hemorrhagic syndrome [9].WHO statistics confirm that 71 million people worldwide have a chronic HCV infection. The main risk is that 55% to 85% of patients with acute HCV infection develop a chronic form, which is the leading cause of liver cirrhosis and the need for transplantation [6,9,10].Purpose of the study. The aim of this study was to evaluate the clinical efficacy of a comprehensive treatment and prevention protocol specifically designed for patients suffering from chronic diffuse liver diseases.
2. Materials and Methods
- Taking into account various principles of modern scientific knowledge, we have developed our research methodology with a sufficiently defined objective. Planned and conducted research based on general scientific and specific methods was aimed at solving the set tasks. Within the framework of this study, 94 patients with chronic diffuse liver disease (CDL) were included. The control group consisted of 23 conditionally healthy patients. In turn, patients with JSDK were divided into 3 groups depending on the type of disease.In turn, patients were further divided into 2 groups according to the treatment method: group I (n=44): traditional dental treatment. Group II (n=50): comprehensive treatment (Rotokan preparation and physiotherapy in addition to traditional treatment).For the purpose of traditional dental treatment, traditional mechanical cleaning and filling of carious tooth cavities with standard filling materials, standard antiseptic treatment and filling of the root canals, cleaning of the oral cavity from dental stones and deposits using traditional methods, and treatment of the gums and periodontal tissues with standard anti-inflammatory ointments, gels (Metrogil Denta), and antiseptics were performed.In complex treatment, in addition to traditional treatment, liquid extract of the medicinal plant Rotokan (composition: extract of chamomile, carnation, and buckwheat) and physiotherapy (electrophoresis with Vitamin C and ultra-high frequency therapy) were used.Rotokan is not used in its pure form; it was diluted with water before use. 1 teaspoon (5 ml) of Rotokan was dissolved in 1 cup (200 ml) of warm water. It was prescribed to be rinsed 3-4 times a day for 1-2 minutes. The cotton swab (turunda) is dipped in the solution and placed on the gum margin for 15-20 minutes. The water temperature must be 35-40°C, as cold water can increase vascular spasms observed in liver pathology, while very hot water can increase bleeding. Course duration: 7–10 days. A total of 5–15 treatments (depending on the severity of the disease).For the purpose of physiotherapy (electrophoresis), a 5% ascorbic acid solution was used. Cotton swabs moistened with the solution are placed on the gums and connected to the anode (+) pole. Current strength: 2...5 mA (depending on the patient's individual sensitivity, up to a "light itch" sensation). The first procedures begin at 10 minutes and are gradually increased to 15-20 minutes. Course duration: 10-12 treatments, daily or every other day. Ultra-high frequency therapy (UHF). An oligothermic dose (where weak heat is felt) is used. The power for the jaw area was set at around 20-30 W. Bilaterally or transversely to the affected area of the jaw. Air gap 1...1.5 cm. Duration: 8–10 minutes. Course duration: 5–8 treatments.It is recommended to perform these two procedures on the same day, one after the other, to achieve the maximum effect in LSDK. First, UVCH therapy: this procedure generates heat in the tissues, dilates the capillaries, and accelerates blood flow. After UVCH, tissue permeability increases, resulting in better absorption of ascorbic acid into the deep layers of the periodontium.
3. Results and Discussion
- The patients were analyzed by age categories, and the results are shown in Table 1. The distribution of the 94 patients participating in the study by type of liver pathology and the treatment methods used indicates a consistency between the groups. Specifically, out of 35 patients with liver fibrosis, 45.7% (16 patients) were assigned to Group I with comprehensive treatment, while 54.3% (19 patients) were assigned to Group II with traditional treatment.
|
|
|
|
4. Conclusions
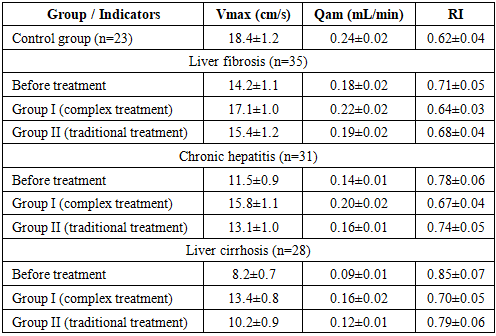
- The conducted study demonstrated that in patients with chronic diffuse liver diseases, the severity of hepatic pathology is directly associated with deterioration of periodontal status, including worsening hygienic indices (GI), increased inflammatory activity (PMA), decreased enamel resistance (TER), and higher caries intensity (KE). Additionally, Doppler ultrasonography findings revealed significant impairment of periodontal microcirculation, characterized by reduced blood flow velocity (Vmax), decreased volumetric blood flow (Qam), and increased vascular resistance (RI), which indicates the development of ischemic-hypoxic processes in periodontal tissues. These findings confirm the systemic impact of liver pathology on oral health and substantiate the pathogenetic link between hepatic dysfunction and periodontal tissue damage.The application of the developed comprehensive treatment approach, including herbal therapy (Rotokan) and physiotherapeutic modalities (vitamin C electrophoresis and UHF therapy), demonstrated significantly higher clinical efficacy compared to conventional dental treatment. This was evidenced by a more pronounced improvement in periodontal indices, restoration of enamel resistance, stabilization of caries progression, and normalization of microcirculatory parameters (Vmax, Qam, RI). The obtained results scientifically substantiate that a multidisciplinary, pathogenetically oriented treatment strategy plays a decisive role in improving therapeutic outcomes and preventing complications in patients with chronic diffuse liver diseases.