-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2179-2181
doi:10.5923/j.ajmms.20261604.128
Received: Mar. 20, 2026; Accepted: Apr. 24, 2026; Published: Apr. 29, 2026

Assessment of Renal Blood Flow and Hemodynamics in Pregnant Women According to the Severity of Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. K. Ahmedov1, G. M. Axmadjonova2, G. B. Asxanova2
1Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan
2Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Preeclampsia is a multisystem disorder of pregnancy characterized by significant hemodynamic and metabolic disturbances, particularly affecting renal function. The present study aimed to assess renal blood flow and intrarenal hemodynamics in pregnant women depending on the severity of preeclampsia, as well as to evaluate the prognostic significance of biochemical markers, especially serum uric acid. A total of 130 pregnant women at 34–42 weeks of gestation were included and divided into three groups: physiologically normal pregnancy (control), moderate preeclampsia, and severe preeclampsia. Renal blood flow was assessed using Doppler ultrasonography, with particular emphasis on the resistive index (RI) in segmental and interlobar arteries. The results demonstrated no significant differences in large renal vessels; however, a statistically significant increase in RI was observed in intrarenal arteries with increasing disease severity (p < 0.01–0.001). Serum uric acid levels showed a marked elevation in patients with preeclampsia, reaching the highest values in severe cases (p < 0.001). Correlation analysis revealed a strong positive relationship between serum uric acid and renal vascular resistance (r = +0.71; p < 0.001). These findings indicate that renal hemodynamic impairment and metabolic disturbances progress in parallel with the severity of preeclampsia. The combined use of Doppler-derived indices and biochemical markers, particularly uric acid, provides valuable diagnostic and prognostic information for early risk stratification and management of preeclampsia.
Keywords: Preeclampsia, Renal hemodynamics, Resistive index, Doppler ultrasonography, Uric acid, Renal blood flow, Vascular resistance, Pregnancy complications, Microcirculation, Risk stratification
Cite this paper: F. K. Ahmedov, G. M. Axmadjonova, G. B. Asxanova, Assessment of Renal Blood Flow and Hemodynamics in Pregnant Women According to the Severity of Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2179-2181. doi: 10.5923/j.ajmms.20261604.128.
1. Introduction
- Preeclampsia represents a multisystem disorder of pregnancy in which functional disturbances develop across several maternal organs. Among these, the kidneys play a central and early role, as they are particularly sensitive to hemodynamic and vascular alterations that characterize this condition [1,3,4,5].The clinical severity of preeclampsia and its consequences for both the mother and the fetus are largely determined by the extent of renal involvement. The underlying mechanisms are closely related to systemic vascular dysfunction, primarily manifested by persistent vasoconstriction and endothelial damage. These changes impair tissue perfusion, including uteroplacental circulation, and significantly reduce renal blood flow. As a result, glomerular filtration declines, leading to progressive renal dysfunction, which is clinically reflected by the development of proteinuria [8].In the setting of widespread vasospasm and ischemic processes, metabolic disturbances also become evident. One of the most informative indicators is an increase in serum uric acid, the final product of purine metabolism, with levels exceeding 5.5 mg% considered clinically significant. Uric acid metabolism is closely linked to hepatic synthesis and renal excretion pathways [1,3]. Therefore, elevated plasma levels, particularly when accompanied by reduced urinary elimination, can be interpreted as a marker of impaired renal function and an early sign of hypertensive complications during pregnancy [2,4,6].Given that hyperuricemia develops through multiple pathophysiological pathways, its clinical relevance has been widely investigated. According to K.P. Williams and T. Gallernoau (2002), uric acid levels above 5.5 mg% during pregnancy are strongly associated with the onset of hypertensive disorders and an increased likelihood of adverse perinatal outcomes. Similar observations were reported by V.C. Warwe and O.O. Abudu (1999), who demonstrated that elevated uric acid concentrations can serve as a useful criterion for identifying women at high risk of developing preeclampsia [6,7,8].Thus, the evaluation of renal hemodynamics together with biochemical markers, particularly uric acid, provides valuable insight into the pathogenesis and progression of preeclampsia. This approach enhances early risk stratification and improves the prediction of both maternal and fetal complications.Aim of the study.To assess renal blood flow and systemic hemodynamic changes in pregnant women depending on the severity of preeclampsia, and to determine the prognostic significance of biochemical markers, particularly serum uric acid, in the early identification and risk stratification of maternal and fetal complications.
2. Materials and Methods
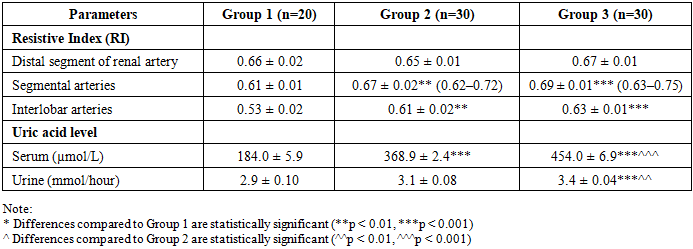
- The present study was conducted to evaluate renal function and renal hemodynamics in pregnant women at late gestational stages. A total of 130 pregnant women at 34–42 weeks of gestation were enrolled. The study population was stratified into three groups according to the clinical course and severity of preeclampsia.The control group (Group I) consisted of 20 women with physiologically uncomplicated pregnancies. Group II included 30 pregnant women diagnosed with moderate preeclampsia, while Group III comprised 30 patients with severe preeclampsia.In all groups, renal blood flow was assessed using Doppler ultrasonography during the third trimester (34–42 weeks of gestation). The examination was performed with duplex scanning techniques combining pulsed-wave and color Doppler modes, which allowed a detailed evaluation of intrarenal hemodynamics.Considering the wide range of Doppler-derived parameters and the pathophysiological features of preeclampsia—particularly the predominance of increased vascular resistance and generalized vasospasm—it was deemed methodologically appropriate to focus on indices reflecting vascular resistance. In this context, special emphasis was placed on the resistive index (RI) as the most informative parameter for characterizing renal vascular tone.To assess intrarenal vascular resistance, RI values were measured at the level of segmental and interlobar arteries within the distal portions of the renal arterial tree. This approach enabled a more precise evaluation of changes in renal perfusion associated with varying severity of preeclampsia.The table summarizes the results of renal vascular resistance assessment in pregnant women with uncomplicated pregnancies and those diagnosed with moderate and severe forms of preeclampsia.
|
3. Conclusions
- The severity of preeclampsia is associated with a progressive increase in intrarenal vascular resistance, particularly at the level of segmental and interlobar arteries, where the resistive index rises from 0.61±0.01 and 0.53±0.02 in physiological pregnancy to 0.69±0.01 and 0.63±0.01 in severe cases (p<0.001), indicating significant impairment of renal microcirculation. Serum uric acid levels demonstrate a marked and statistically significant elevation with increasing severity of preeclampsia (from 184.0±5.9 µmol/L to 454.0±6.9 µmol/L; p<0.001), confirming its role as a reliable biochemical marker of disease progression and renal dysfunction. A strong positive correlation between serum uric acid and renal vascular resistance (r=+0.71; p<0.001), along with a significant association confirmed by chi-square analysis (χ²=12.4; p<0.01), indicates that hemodynamic and metabolic disturbances are closely interconnected and can be effectively used for risk stratification and prognostic assessment in preeclampsia.