-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2176-2178
doi:10.5923/j.ajmms.20261604.127
Received: Mar. 25, 2026; Accepted: Apr. 24, 2026; Published: Apr. 29, 2026

Thyroid Index in Patients with Vitiligo
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhamidova Farida Muinovna, Toshev Suhrob Uktamjon ugli
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Vitiligo is a chronic autoimmune skin disorder characterized by progressive destruction of melanocytes, leading to depigmented skin lesions. Increasing evidence suggests that autoimmune thyroid diseases are among the most common comorbid conditions associated with vitiligo. Thyroid hormones, including triiodothyronine (T3) and thyroxine (T4), play an important role in regulating cellular metabolism, proliferation, differentiation, and immune homeostasis. Thyroid-stimulating hormone (TSH) regulates thyroid function via a negative feedback mechanism and serves as a sensitive marker of thyroid dysfunction. Assessment of thyroid status in patients with vitiligo is clinically relevant, as thyroid dysfunction may influence disease progression and therapeutic outcomes. For a more comprehensive evaluation of thyroid hormonal activity, an integral thyroid functional index (TTF = T3 × T4) can be used.
Keywords: Vitiligo, Thyroid hormones, T3, T4, TSH, Thyroid functional index, TTF, Autoimmune diseases, Hypothyroidism
Cite this paper: Khamidova Farida Muinovna, Toshev Suhrob Uktamjon ugli, Thyroid Index in Patients with Vitiligo, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2176-2178. doi: 10.5923/j.ajmms.20261604.127.
1. Introduction
- The thyroid gland is involved in important vital processes of the body, it regulates the process of metabolism, division and differentiation of cells in the body, and also regulates the normal functioning of the immune status of the body. The key hormones of the thyroid gland are thyroxine (T4) and triiodothyronine (T3), whose function is to enhance metabolism, synthesize proteins and regulate fat and carbohydrate metabolism. A more active form of hormones synthesized in the thyroid gland is T3, since it is formed directly in the gland itself, T4 unlike T3, is formed as a result of peripheral generation [1,3].The thyroid gland itself is regulated by thyroid-stimulating hormone (TSH), which is synthesized in the pituitary gland. TSH balances the secretion and production of thyroid hormones through a negative feedback mechanism. This is achieved by increasing the secretion of TSH while decreasing the concentration of thyroid hormones, thereby enhancing the secretory function of the thyroid gland itself. Also, an increase in the concentration of T3 and T4 in the blood reduces the release of TSH, thereby inhibiting secretion in the thyroid gland [4,6].Thyroid dysfunction is common in the population and can manifest as hypothyroidism or hyperthyroidism. Disruptions in normal thyroid function can impact the course of various diseases, including dermatological ones, and affect the effectiveness of treatment. Based on this, the determination of concentrations of T3, T4 and TSH is important for determining the pathogenesis and increasing the effectiveness of treatment of diseases, including dermatological ones [2,5].To determine the overall impact of thyroid hormones on the body, it is advisable to use a complex indicator that determines the overall impact of thyroid hormones: TTF = T3 × T4 [4].Objective of the study: Determination and comprehensive assessment of the thyroid gland condition based on the concentration of thyroid hormones and TSH by integrating the thyroid index (TTF).
2. Materials and Methods
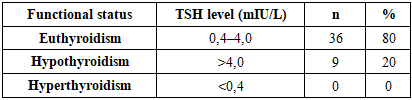
- The study involved 45 patients diagnosed with vitiligo, whose serum T3, T4, and TSH levels were measured. The studies were conducted exclusively using accepted clinical protocols and standard immunoassay and chemiluminescent methods. Statistical analysis of the data was performed using a descriptive method.Statistical processing of the obtained results was performed using descriptive statistics. For quantitative indicators, the mean (M), standard deviation (SD), median (Me), interquartile range (Q1–Q3), and minimum and maximum values were calculated.Standard TSH levels in the blood range from 0.4 to 4.0 mIU/L. A TSH level of 4.0 or higher can be considered a laboratory indicator of possible hypothyroidism, while a level of 0.4 or lower may indicate increased thyroid function (hyperthyroidism).
3. Results
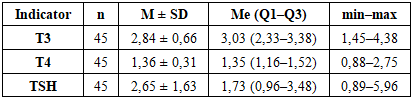
- The analysis revealed that the average triiodothyronine (T3) level in the examined patients was 2.84 ± 0.66, with a median of 3.03 (2.33–3.38). The minimum value was 1.45, and the maximum was 4.38. These data indicate that, on average, T3 levels were within physiological limits.The mean thyroxine (T4) concentration was 1.36 ± 0.31, with a median of 1.35 (1.16–1.52). The minimum and maximum T4 values were 0.88 and 2.75, respectively. Overall, T4 levels showed moderate variability and were within the reference range in most patients.The mean thyroid-stimulating hormone (TSH) level was 2.65 ± 1.63 mIU/L, the median was 1.73 (0.96–3.48). The minimum TSH value was 0.89 mIU/L, the maximum was 5.96 mIU/L, indicating the presence of isolated cases of deviation from physiological values (Table 1).
|
|
4. Conclusions
- In the majority of patients examined, thyroid hormone levels (T3 and T4) were within physiological norms, and the average thyroid-stimulating hormone (TSH) level was 2.65 ± 1.63 mIU/L, corresponding to a euthyroid state. This indicates that baseline thyroid hormone activity was maintained in the majority of the sample.Elevated TSH levels (>4.0 mIU/L) were detected in 20% of patients, which may indicate subclinical hypothyroidism. Such changes require clinical monitoring, as, if left uncorrected, they can progress to overt hypothyroidism and impact metabolic processes and overall health.Calculating the integrated thyroid function index (TTF = T3 × T4) allowed for a comprehensive assessment of the total hormonal activity of the thyroid gland. TTF values were within normal limits in most patients, confirming the maintenance of overall functional activity even with isolated TSH deviations.A comprehensive laboratory assessment of thyroid status using T3, T4, TSH and TTF is an informative tool for early detection of subclinical disorders, dynamic monitoring of thyroid status and timely clinical decision-making.To improve the accuracy of diagnosis and assessment of the functional activity of the thyroid gland, further research with an expanded sample of patients, including different age and gender groups, as well as an assessment of the relationship of TTF indicators with clinical manifestations and concomitant diseases is recommended.