-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1608-1612
doi:10.5923/j.ajmms.20261604.12
Received: Mar. 6, 2026; Accepted: Mar. 27, 2026; Published: Apr. 1, 2026

Optimal Timing for Minor Foot Surgery After Peripheral Artery Revascularization in Patients with Diabetic Foot Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMatmurotov K. J.1, Narmetov A. B.2, Sapayev B.3
1Tashkent State Medical University, Uzbekistan
2Khorezm Branch of the Republican Specialized Scientific-Practical Medical Center of Endocrinology, Uzbekistan
3Alfraganus University, Uzbekistan
Correspondence to: Matmurotov K. J., Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This research paper analyzed the results of treatment of 157 patients with purulent-necrotic lesions of the foot in patients with diabetic foot syndrome against a background of severe tissue ischemia, who underwent various types of foot surgery. Depending on the surgical treatment strategy, patients were divided into two groups. The first group (comparison) consisted of 82 (52.2%) patients who received inpatient treatment in 2020-2022. These patients underwent surgical interventions using the traditional method, without taking into account the nature of ischemia and clear criteria for the timing of the operation. The second group, which was considered the main one, included 75 (47.8%) patients who were treated in 2023-2025. The surgical treatment tactics in this group differed sharply from those in the comparison group, with the optimal choice of the timing of surgical treatment and the specifics of reconstructive and plastic surgery on the foot.
Keywords: Diabetes mellitus, Gangrene, Amputation, Endovascular revascularisation
Cite this paper: Matmurotov K. J., Narmetov A. B., Sapayev B., Optimal Timing for Minor Foot Surgery After Peripheral Artery Revascularization in Patients with Diabetic Foot Syndrome, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1608-1612. doi: 10.5923/j.ajmms.20261604.12.
Article Outline
1. Introduction
- Diabetes mellitus is the most common endocrine disease in the world. According to IDF Diabetes, in 2024 there were 589 million people with diabetes among the population aged 20-79 worldwide, and it is predicted that by 2050, 853 million people will suffer from diabetes mellitus [1,10,14]. According to statistics for 2023, 3,845,176 patients in our country were diagnosed with type 2 diabetes [2,11,13,20]. Specialists have been regularly studying diabetes mellitus and its complications for the last 20-30 years. During this time, various theories of the etiopathogenesis of DM have been proposed, and the main factors in the development of the disease have been identified. Towards the end of the 20th century, most scientists reached a consensus that diabetes mellitus involves a number of tissues, organs, and systems in the pathological process. One of the most serious and dangerous complications of diabetes is damage to the lower extremities [3,7,18,21]. Multifocal damage to target organs is directly related to a reduction in the diameter of the artery lumen, up to its complete closure, which causes a significant disruption in the blood supply to the main vessels, leading to impaired blood circulation in the microcirculatory vessels and causing tissue hypoxia and tissue metabolism disorders. The situation is exacerbated by the opening of shunting arteriolar-venular anastomoses. This effect is relevant in the development of skin and muscle ischemia. As a result of a complex imbalance in the coagulation system, disseminated intravascular coagulation develops, which subsequently leads to the development of destructive changes in tissues under conditions of hypoxia [4,9,12,17].The main cause of peripheral arterial disease is atherosclerosis, but in the context of diabetes mellitus, the pathophysiological process aimed at changing the vascular bed is also of considerable importance. At the same time, a number of other nosologies associated with gradual obliteration of the arteries can cause chronic limb ischemia syndrome. The following are among the main risk factors [1,5,18].The prevalence of occlusive-stenotic peripheral artery disease, whether symptomatic or asymptomatic, is slightly higher among men than women, particularly in younger age groups. Among patients with intermittent claudication, the ratio of men to women ranges from 1:1 to 2:1. As discussed in the previous section on epidemiology, the incidence and prevalence of diseases related to arteries increase sharply with age [6,8,11,15,19]. It is one of the main risk factors for the development of peripheral arterial disease. It contributes to the development of this disease 2-3 times more often than cardiovascular disease. Large randomised epidemiological studies have revealed that smoking increases the risk of developing PAD by 2-6 times and IC by 3-10 times [7,10,16,21].Considering the above-mentioned literature data and despite the development of surgical technologies in this area, the frequency of high amputations and mortality rates has not decreased. One important factor in the treatment of patients with gangrene is the optimal timing of debridement surgery after adequate revascularization. In this regard, we decided to study this issue and offer our assessment of how to solve this problem.The aim of this study was to improve the results of surgical treatment of purulent-necrotic lesions against a background of severe ischemia in patients with diabetic foot syndrome.
2. Materials and Methods
- This research paper analyzed the results of treatment of 157 patients with purulent-necrotic lesions of the foot in patients with diabetic foot syndrome against a background of severe tissue ischemia, who underwent various types of foot surgery. The patients under study were hospitalized in the purulent surgery department of the Tashkent Medical Academy's multidisciplinary clinic and the Twins Medical Center private clinic in 2020-2025. Depending on the surgical treatment strategy, patients were divided into two groups. The first group (comparison) consisted of 82 (52.2%) patients who received inpatient treatment in 2020-2022. These patients underwent surgical interventions using the traditional method, without taking into account the nature of ischemia and clear criteria for the timing of the operation.The second group, which was considered the main one, included 75 (47.8%) patients who were treated in 2023-2025. The surgical treatment tactics in this group differed sharply from those in the comparison group, with the optimal choice of the timing of surgical treatment and the specifics of reconstructive and plastic surgery on the foot.The data obtained during the study showed that patients had a much more severe clinical condition upon admission. Among the patients examined during their initial visit to the hospital, 56 (35.7%) of 157 had total foot ischemia with signs of partial foot muscle contracture. Indeed, this condition complicated our tasks in terms of choosing surgical procedures and preserving the musculoskeletal function of the lower limb as a whole. Severe foot ischemia without any trophic disorders was observed in only 5 cases (3.2%), which was treated conservatively after revascularization of the peripheral arteries. Distal gangrene involving the toes was observed in 40 patients (25.5%). Of course, the primary goal in treating severe foot ischemia is to preserve the feet or the weight-bearing function of the limb in patients with diabetic foot syndrome, but an initial incorrect or inadequate surgical strategy can worsen the situation, leading to limb loss or death. In patients, using non-invasive and invasive methods of studying the condition of the peripheral arterial bed, the severity of mediocalcinosis development was determined, which determines the degree of ischemia in the foot. Calcification of arterial walls is a gross metabolic disorder against the background of diabetes mellitus, which is not uncommon in patients with diabetic foot syndrome. Our study included patients with pronounced foot ischemia and these patients did not have I-degree mediocalcinosis. According to the examination data, only II and III degrees of arterial wall damage were observed in patients.
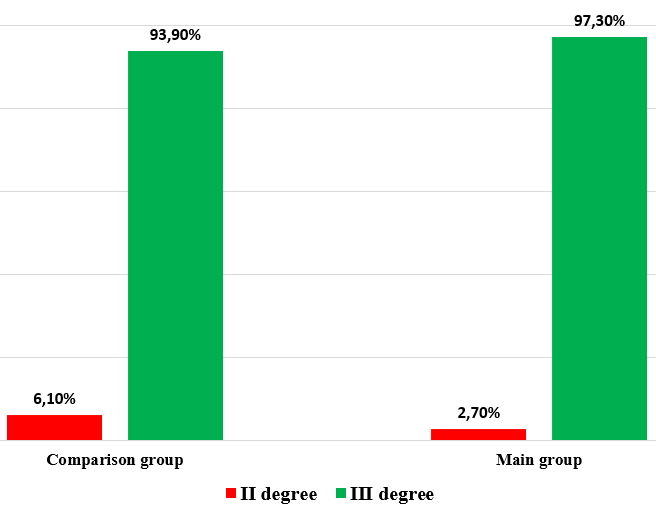 | Figure 1. Severity of medial calcification of the arteries of the lower extremities |
3. Results and Discussion
- In our study, the control group consisted of 85 patients who underwent endovascular revascularization procedures for purulent-necrotic lesions. Conservative treatment consisted of eliminating factors that could further worsen arterial blood supply to the lower extremities. Simultaneous correction of blood lipid and glucose levels was also performed.Drug treatment included the prescription of dual anticoagulant therapy and prostaglandin E1 (vasostenon). Along with systemic vascular therapy, patients underwent local therapy, which included modern dressing preparations and, of course, vacuum therapy to accelerate the healing process against the background of ischemia relief. Within 10-14 days after the application of these procedures to the infected and trophic wound, its cleansing from detritus and discharge was observed, which directly contributed to the growth of granulation tissue with the transition to the second phase of the wound healing process.Despite adequate treatment, the comparison group continued to experience adverse outcomes associated with a high frequency of amputations and repeat secondary surgical interventions. In our opinion, the main reason for this was the failure to take into account the timing of primary radical surgical interventions on the foot. We consider the simultaneous removal of all necrotic tissues immediately after improving arterial blood flow through endovascular revascularization to be inappropriate, since a minimum of 4-5 days is required for the remodeling of the collateral arterial network (according to our data). Oxygen tension indicators in the postoperative period also confirm our actions.An analysis of the immediate results of surgical treatment in the study groups showed that in the main group, the frequency of good treatment outcomes improved by almost 10%, and high amputation of the lower extremities decreased fourfold. The rate of minor amputations of the foot was higher in the main group than in the comparison group (10.6–14.7%) (see Fig. 2).
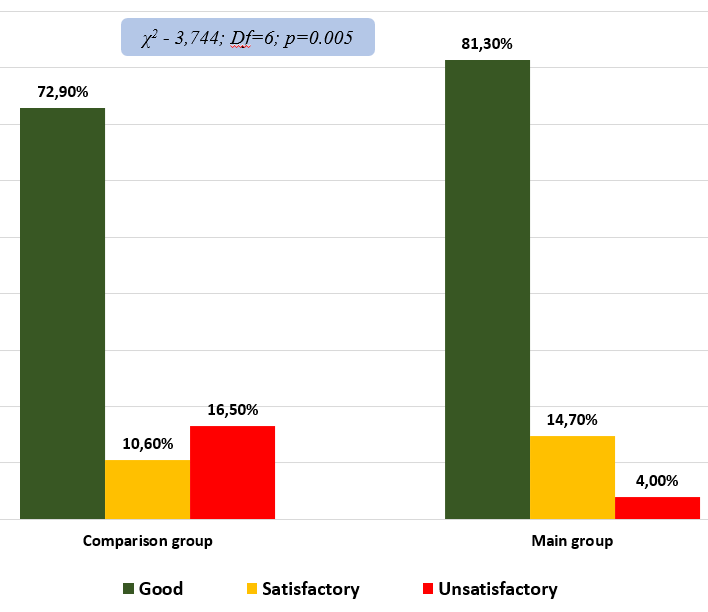 | Figure 2. Comparative analysis of immediate treatment outcomes |
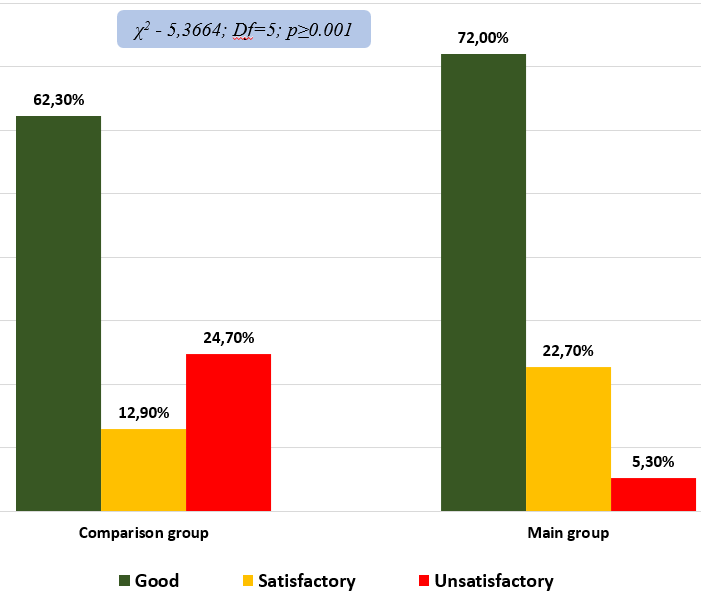 | Figure 3. Comparative analysis of the immediate treatment results |
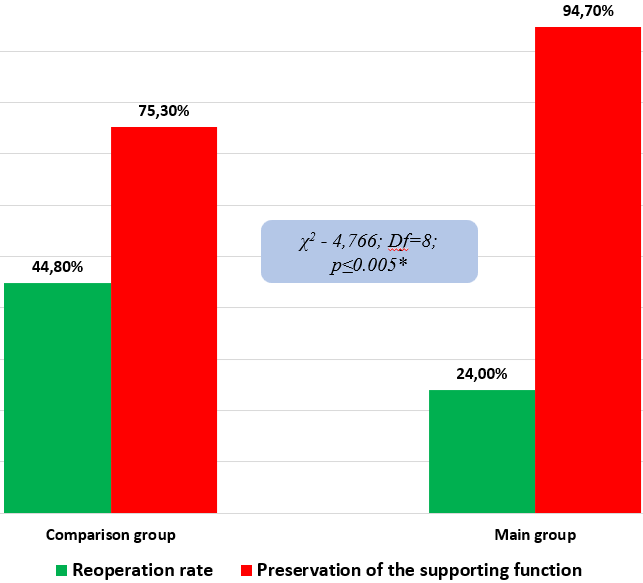 | Figure 4. Comparative characteristics of the effectiveness of surgical tactics |
4. Discussion
- Drug treatment included the prescription of dual anticoagulant therapy and prostaglandin E1 (vasastenon). Along with systemic vascular therapy, patients underwent local therapy, which included modern dressing preparations and, of course, vacuum therapy to accelerate the healing process against the background of ischemia relief. Within 10-14 days after the application of these procedures to the infected and trophic wound, its cleansing from detritus and discharge was observed, which directly contributed to the growth of granulation tissue with the transition to the second phase of the wound healing process.Despite adequate treatment, the comparison group continued to experience adverse outcomes associated with a high frequency of amputations and repeat secondary surgical interventions. In our opinion, the main reason for this was the failure to take into account the timing of primary radical surgical interventions on the foot. We consider the simultaneous removal of all necrotic tissues immediately after improving arterial blood flow through endovascular revascularization to be inappropriate, since a minimum of 4-5 days is required for the remodeling of the collateral arterial network (according to our data). Oxygen tension indicators in the postoperative period also confirm our actions. Our study has some limitations. We performed a retrospective analysis of a prospectively observed cohort from a single department. The choice of endovascular revascularization treatment was not randomized. Ischemic wounds were not stratified according to their location and extent. Finally, ambulatory status was not assessed prior to revascularization.
5. Findings
- 1. After revascularization and surgical interventions on the foot in the long term, the optimal condition for reconstructive surgery is considered to be tсрО2<35.4±4.6 mmHg. For the use of VAC therapy after reconstructive surgery (with local tissues or autodermoplasty), the transcutaneous oximetry index should be higher than tсрО2<39.7±9.3 mmHg. 2. In cases of distal tissue damage, the optimal time for foot surgery is on the third day, with oxygen tension reaching tсрО2 - 35.4±9.6 mmHg on the day of revascularization. Restoration of blood flow in cases of total foot ischemia only on the 6th-7th day leads to an increase in the transcutaneous oximetry index to tсрО2 - 34.8±5.7. In wet gangrene, after opening the lesion on the 5th day after revascularization, oxygen tension increases to tсрО2 - 34.5±8.3, which makes it possible to perform necrectomy.3. Using improved surgical techniques with optimal timing of foot surgery, it was possible to reduce the frequency of repeat operations from 44.8% to 24.0% (p≤0.001) and increase the number of patients with preserved musculoskeletal function of the lower extremities from 75.3% (in the comparison group) to 94.7% (in the main group) (p≤0.005).
Consent
- It is not applicable.
Ethical Approval
- It is not applicable.
Competing Interests
- Authors have declared that no competing interests exist.