Bebutov Feruz Axmedovich1, Axmedov Alibek Baxodirovich2
1Termez Branch of Tashkent State Medical University, Termez, Uzbekistan
2Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Axmedov Alibek Baxodirovich, Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Among the chronic diseases of the gastrointestinal tract in children, lesions of the upper digestive tract are in the first place, including GERD. The medical and social significance of this problem lies in the fact that in most cases, chronic gastroduodenal pathology, which began in childhood, leads to disability of the adult population. Therefore, a large number of publications are devoted to this pathology. However, most authors point to the lack of knowledge of the problem associated with the difficulties of diagnosing this nosological form in children.
Keywords:
Gastroesophageal reflux disease, Children, Oral cavity, Enamel erosion, Dental hyperesthesia, Caries, Periodontal disease
Cite this paper: Bebutov Feruz Axmedovich, Axmedov Alibek Baxodirovich, Functional Characteristics of Erosive Lesions of Dental Hard Tissues in Children with Gastroesophageal Reflux Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2123-2126. doi: 10.5923/j.ajmms.20261604.115.
1. Introduction
In recent years, erosive lesions of the hard tissues of teeth have been considered as one of the most significant problems of pediatric dentistry, due to their high prevalence, irreversible nature of enamel loss and pronounced impact on the quality of life of patients. Special attention in modern research is paid to exogenous and endogenous acid factors, among which gastroesophageal reflux disease (GERD) occupies a leading position. Regular exposure of gastric contents with low pH to the structures of the oral cavity leads to demineralization of enamel, a decrease in its resistance and the formation of erosive defects, especially in primary school children, whose enamel is characterized by functional immaturity. According to modern data, diseases of the gastrointestinal tract occupy one of the first places in the structure of somatic pathology in children and tend to increase. The frequency of diseases of the digestive system among the children's population of Ukraine is second only to diseases of the respiratory system and amounts to 117.07 per 1000 population. Interest in this pathology exists in other countries, which underlines the urgency of the problem [2,4,6,8,10,12,14].The purpose of the study. Assessment of the clinical and functional features of the dental status and the prevalence of erosive lesions of the hard tissues of teeth in children with gastroesophageal reflux disease based on a comprehensive clinical examination and questionnaire.
2. Materials and Methods
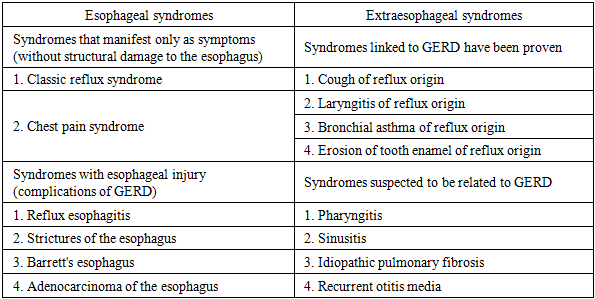
85 children with signs of erosive dental lesions on the background of GERD were examined. The analysis included an assessment of the BEWE index, oral hygiene indicators (OHI-S, API), carious status (DMFT/dmft), oral fluid parameters (pH, buffer capacity, salivation rate), as well as data from a survey of doctors and parents. Additionally, subjective gastrointestinal and dental complaints were studied. Results. The average age of the surveyed was 8.5±0.77 years, and the gender distribution was uniform. The frequency of erosive lesions was 34%, while the average BEWE index reached 4.2± 0.41 points, indicating the predominance of mild and moderate forms of erosion. The average stage of BEWE (1.12±0.01) corresponded to the initial lesion level, which is typical for the pediatric population of this age group.The clinical course of GER in children is characterized by pain, dyspeptic, asthenovegetative and respiratory syndromes, and may vary depending on the age of the child. • In young children, symptoms predominate: vomiting, refusal to eat, weight gain lag, irritability, regurgitation, apnea. • In older children, abdominal pain, heartburn, vomiting, regurgitation, dysphagia (difficulty swallowing), night cough are more common. In both age groups, one of the first symptoms may be frequent and prolonged hiccups. In addition, GERD can lead to sleep disorders and a child's psychosocial status. In the structure of clinical manifestations of GERD in children, as in adults, there are: • Esophageal symptoms: heartburn, regurgitation, "wet spot" symptom, belching, dysphagia (pain when swallowing), dysphagia.• Extraesophageal symptoms: manifestations from the bronchopulmonary system, oral cavity, ENT organs, etc. More than 60% of children suffering from GERD complain of dull pain in the epigastric region and behind the sternum, which occurs immediately after eating, increases with torso bends and weakens after 1.5–2 hours. However, it is in childhood that extraesophageal symptoms often come to the fore.: • bronchopulmonary system, • oral cavities, • ENT organs, which is explained by the common embryological origin and anatomical connection between the respiratory, digestive and cardiovascular systems. Extraesophageal symptoms, the mechanism of which is the direct contact of the mucous membranes of the upper and lower respiratory tracts, as well as the oral cavity with gastric or gastrointestinal contents due to its casting above the upper esophageal sphincter, indicate the development of pathological processes in the ENT organs, bronchopulmonary, cardiovascular systems and in the oral cavity. When describing extraesophageal symptoms, most authors usually primarily consider bronchopulmonary disorders associated with GERD, as they are more studied and known to practitioners, undeservedly relegating the dental manifestations of GERD to the background.Table 1. Clinical syndromes associated with GERD (Montreal, 2005)
 |
| |
|
The hygienic condition of the oral cavity was assessed as satisfactory: the OHI-S index was 1.7±0.01 points, API — 48%. The carious status was characterized by moderate dental lesions (DMFT/dmft = 1.2/2.3). The functional parameters of saliva indicated the presence of unfavorable factors: the average salivation rate (0.45±0.02 ml/min) was lower than the reference values, and 18.5% of children complained of dry mouth. One of the important and insufficiently studied issues of pediatric gastroenterology remains the study of factors influencing the nature of the course and development of complications in chronic gastroduodenal pathology [1,3,5,7,9,11,13,14]. The development and course of gastrointestinal diseases largely depend on the individual genetic profile of the patient, therefore, the study of the relationship of molecular genetic markers with the occurrence and development of dental diseases in children with GERD is relevant for the development of individual preventive programs.There is evidence of the effect of the type III collagen gene (COL3A1) on the development of gastroesophageal reflux; in addition, mutations of this gene are associated with abnormalities of the oral cavity and teeth. The COL3A1 gene encodes type III collagen— a fibrillar extracellular matrix protein present in connective tissue with stretchable properties. The accumulation of type III collagen is a sign of chronic diseases, including fibrotic processes. The literature describes the differential expression of COL3A1 in biopsies of the esophagus of patients with GERD compared with healthy ones. Disruption of collagen III production by gum fibroblasts leads to a tendency to bleeding. Determination of predisposition to GERD at the molecular genetic level makes it possible to prevent the development of dental complications of gastroesophageal reflux in children. From a theoretical point of view, GERD is a form of the disease in which it is difficult to separate the etiology and pathogenesis. Considering the main factors of GERD in children, it is necessary to pay attention to the anatomical and physiological features of the development and functioning of the digestive tract of the child. It should be noted that in this category of patients, the disease is most often associated with immaturity of the lower esophageal sphincter, which leads to pathological reflux of both acidic and alkaline contents. Therefore, GERD is more often observed in young children, since there are anatomical and physiological prerequisites in this age category. Nevertheless, according to some authors, the general group of factors for the development of GERD in children also includes: obesity, bad habits, decreased physical activity, and dietary habits. As for the sex differences in the development and course of GERD in children, the researchers did not find any definite patterns. There were also no significant differences in the frequency and structure of esophageal complaints among children and adolescents from cities of different sizes.There is no consensus in the literature regarding the association of GERD with Helicobacter pylori infection. Some authors point to a high percentage of infection in this category of patients against the background of acquired immunodeficiency, manifested by T- and B-lymphopenia and a decrease in serum IgA levels. However, other researchers have not established a link between GERD and Helicobacter pylori. In addition, modern publications discuss the role of herpes, cytomegalovirus infection and fungal lesions among the factors contributing to GERD. GERD traditionally refers to acid-dependent diseases, where hydrochloric acid is the main aggressive factor. However, its development is based on a violation of the motility of the upper gastrointestinal tract, namely, a decrease in the contractile function of the lower esophageal sphincter, a decrease in the activity and duration of esophageal clearance, and a slowdown in the evacuation of gastric contents. An imbalance between the parasympathetic and sympathetic parts of the autonomic nervous system, which regulate the work of the gastrointestinal tract, leads to motor disorders of the esophagus and stomach, which many authors are inclined to do based on their own research. In children, especially infants, physiological gastroesophageal reflux (GER) is more common than in adults. This is due to the physiological features of the sphincter and valve apparatus of the cardia, as well as the mechanisms of neurohumoral regulation. As a rule, GER in children in the first months of life has no clinical consequences and often resolves spontaneously when an effective anti-reflux barrier is gradually formed. In older children, GER may also be of a physiological nature and occur normally. Under physiological conditions, the resulting gastroesophageal reflux is quickly eliminated due to esophageal clearance, in which saliva containing bicarbonates plays a role. Therefore, it is believed that pathological reflux develops under conditions of predominance of aggressive factors over protective ones. There is also evidence in the literature on the role of certain hormones in the pathogenesis of GERD, in particular, an increase in cortisol levels has been identified, causing an imbalance between aggressive and protective factors, as well as an increase in insulin levels in children with GERD as a compensatory response to catabolic processes. It should be noted that the primary insufficiency of antireflux mechanisms in young children may be based on dysregulation of the esophagus by the autonomic nervous system caused by hypoxia of the fetal or newborn brain. In older children, hormonal changes in puberty, accelerated growth rate, pronounced psycho-emotional stress and stress play a role in the development of GERD, contributing to the early development of autonomic dysfunction. In addition, one of the factors in the development of pathological gastroesophageal reflux in children is abnormalities in the development of the digestive tract, manifested by pseudoobstruction or antiperistaltic activity. Hernia of the esophageal orifice of the diaphragm is a common provoking factor of GERD in adults, but this dependence has not been confirmed in children.It is also important to note that the secretory function of the stomach undergoes physiological changes during the child's ontogenesis. Alkaline reflux prevails in newborns. At an older age, hydrochloric acid and activated pepsin become an aggressive factor. In childhood, acid dependence is associated not so much with hyperacidity as with a violation of the cytoprotective function of the stomach. Therefore, the main mechanism of development of clinical symptoms of GERD in children is an imbalance between aggression factors (hydrochloric acid, pepsin, increased intra-abdominal pressure) and protective factors (anti-reflux barrier of the esophageal mucosa, esophageal peristalsis, salivary gland secretion). Unlike adults, children, who cannot always accurately describe their complaints, most often have non-specific manifestations of gastroduodenal pathology, including GERD, which is why the disease is not diagnosed prematurely. Of course, children's gastroenteritis. Gastroenterology has all modern diagnostic methods, and there are a sufficient number of publications in the literature on the diagnosis of GERD in children. However, each of these methods has both advantages and disadvantages, among which one of the main ones is invasiveness. In this regard, a number of authors in their research used a reflux questionnaire for the initial detection of GERD in children, the prototype of which is an adapted and revised American questionnaire. The analysis of the doctors' questionnaire demonstrated a high consistency of expert assessments with objective clinical data, which confirms the reliability of the results obtained. The children's subjective complaints (tooth sensitivity, sour taste, burning sensation) correlated with the clinical manifestations of erosive changes.
3. Conclusions
The data obtained indicate the high clinical and functional significance of gastroesophageal reflux disease as an endogenous risk factor for the formation of erosive enamel lesions in children. The revealed changes are mainly of an initial nature, which underlines the relevance of early diagnosis and timely preventive intervention. A comprehensive assessment of the dental status in children with GERD should be considered as an indispensable element of an interdisciplinary approach in pediatric practice.
References
| [1] | Abdalov H.V. Improving the effectiveness of treatment of destructive forms of chronic periodontitis: dissertation of the Candidate of medical Sciences / H.V. Abdalov. -Moscow, 1990. - 143 p. |
| [2] | Bazhanov H.H. Bacterial microflora in odontogenic acute purulent diseases of the maxillofacial region / H.H. Bazhanov, E.P. Pashkov, M.S. Kultaev / Dentistry. - 1985. - No. 1. - p. 31. |
| [3] | Barer G.M. The effect of topical application of a complex of antibacterial drugs on the course of chronic periodontitis / G.M. Barer, V.V. Kocherzhinsky, H.A. Ovchinnikova // Clinical dentistry. -1997. -No. 3. - pp. 12-14. |
| [4] | Vershigora A.E. Cellular and molecular foundations of local immunity / A.E.Vershigora, V.V. Ovod // Successes of modern biology. -1981. - Issue 3. - pp. 394-408. |
| [5] | Vinnichenko A.B. Instrumental treatment of root canals in the treatment of apical periodontitis: dissertation of the Candidate of medical Sciences / A.B. Vinnichenko. - Moscow, 1970. 168 p. |
| [6] | Groshikov M.I. Treatment of apical periodontitis / M.I. Groshikov // Dentistry. 1970. No. 2. pp. 66-70. |
| [7] | Gubin M.A. Clinic and treatment of septic shock in dental patients. / M.A. Gubin // Dentistry. - 1980. - No. 1. - pp. 33-35. |
| [8] | Dmitrieva H.A. Purulent-inflammatory complications of the maxillofacial region, the structure of their pathogens and possible ways of prevention: abstract of the dissertation of the Candidate of medical Sciences / H.A. Dmitrieva. - Moscow, 1993. - 17 p. |
| [9] | Dubova M.A. Modern technologies in endodontics: textbook. manual / M.A. Dubova, T.A. Shpak, I.V. Kornetova. - St. Petersburg, 2005. -93 p. |
| [10] | Zhadko R.T. Comparative assessment of the use of various filling materials in the treatment of periodontitis: dissertation of the Candidate of medical Sciences. - Moscow, 1968. 123 p. |
| [11] | Zharkin A.F. Indicators of acupuncture diagnostics in patients with chronic apical periodontitis / A.F. Zharkin, E.A. Magid, H.H. Trigolos // Actual issues of dentistry: collection of articles - Volgograd, 1996. - pp. 76-81. |
| [12] | Zagorodnova S.A. Changes in the composition of the microflora of the carious cavity in deep caries and pulpitis under the influence of Chlorhexidine and pofesin / S.A. Zagorodnova, S.E. Filichkina. Smolensk, 1988. pp. 6-7. |
| [13] | Kazakova Yu.V. Diagnosis and treatment of acute odontogenic inflammatory processes in patients using mathematical modeling and forecasting methods: abstract of the dissertation of the Candidate of Medical Sciences / Yu.V. Kazakova. - Perm, 1991. - 22 p. |
| [14] | Levkovich A.N. Study of the microflora of periapical tissues in the long term of treatment after periodontitis treatment / A.N. Levkovich // Dentistry. - 1986. - No. 2. - pp. 18-19. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML