-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2085-2088
doi:10.5923/j.ajmms.20261604.106
Received: Mar. 26, 2026; Accepted: Apr. 17, 2026; Published: Apr. 25, 2026

Impact of Immunocorrective Therapy on Systemic Immune-Inflammatory Imbalance in Ischemic Heart Disease with Arterial Hypertension
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNarziyev L. A.1, Akhmedov A. T.2
1PhD Student, Bukhara State Medical Institute, Bukhara, Uzbekistan
2PhD., Associate Professor, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Akhmedov A. T., PhD., Associate Professor, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The combined course of ischemic heart disease and arterial hypertension is associated with a high risk of cardiovascular complications and is characterized by complex pathogenetic mechanisms, including systemic immune-inflammatory dysregulation. Despite advances in standard cardiovascular therapy, the role of immune-targeted interventions in this patient population remains insufficiently studied. The aim of this study was to evaluate the impact of immunocorrective therapy on systemic immune-inflammatory imbalance in patients with ischemic heart disease associated with arterial hypertension. The study included 120 patients aged 35–75 years with verified ischemic heart disease and arterial hypertension. Patients underwent comprehensive clinical, functional, laboratory, and immunological assessment, including evaluation of T-lymphocyte subpopulations (CD3⁺, CD4⁺, CD8⁺, CD4/CD8 ratio), immunoglobulin G (IgG), inflammatory markers (hs-CRP, IL-6, IFN-γ), and NT-proBNP levels. Patients were divided into groups depending on the treatment strategy: standard therapy and combined therapy including immunocorrective agents. The results demonstrated that patients with ischemic heart disease and arterial hypertension exhibit a pronounced immune-inflammatory imbalance characterized by increased levels of hs-CRP and IL-6, reduced IFN-γ levels, decreased CD3⁺ and CD4⁺ T-lymphocytes, and a reduced CD4/CD8 ratio, along with compensatory elevation of IgG. The inclusion of immunocorrective therapy in the treatment regimen led to significant improvement in clinical status, reduction in angina frequency, improvement in NYHA and CCS functional classes, and increased exercise tolerance. These changes were accompanied by normalization of immunological parameters, including an increase in CD3⁺ and CD4⁺ levels, restoration of CD4/CD8 balance, reduction of pro-inflammatory cytokines, and a decrease in NT-proBNP levels.
Keywords: Ischemic heart disease, Arterial hypertension, Immunocorrective therapy, Immune-inflammatory imbalance, Cytokines, CD4/CD8 ratio, hs-CRP, IL-6, NT-proBNP
Cite this paper: Narziyev L. A., Akhmedov A. T., Impact of Immunocorrective Therapy on Systemic Immune-Inflammatory Imbalance in Ischemic Heart Disease with Arterial Hypertension, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2085-2088. doi: 10.5923/j.ajmms.20261604.106.
1. Introduction
- Ischemic heart disease (IHD) and arterial hypertension (AH) remain among the leading causes of morbidity and mortality worldwide, accounting for a substantial proportion of cardiovascular deaths and disability. According to global epidemiological data, the coexistence of these conditions significantly worsens clinical outcomes, contributing to accelerated progression of myocardial dysfunction, increased risk of heart failure, and higher incidence of adverse cardiovascular events. Despite considerable advances in pharmacological management, a significant proportion of patients continue to demonstrate persistent symptoms and unfavorable prognosis, suggesting the presence of additional, insufficiently corrected pathogenetic mechanisms [7,9,11].In recent years, increasing attention has been directed toward the role of systemic immune-inflammatory processes in the development and progression of cardiovascular diseases. A growing body of evidence indicates that chronic low-grade inflammation and immune dysregulation play a central role in endothelial dysfunction, atherosclerotic plaque formation, and vascular remodeling. Elevated levels of pro-inflammatory cytokines, including interleukin-6 (IL-6) and high-sensitivity C-reactive protein (hs-CRP), have been shown to correlate with disease severity and predict adverse cardiovascular outcomes. At the same time, alterations in cellular immunity, particularly changes in T-lymphocyte subpopulations (CD3⁺, CD4⁺, CD8⁺) and imbalance of the CD4/CD8 ratio, reflect systemic immune dysregulation and contribute to the progression of ischemic damage [2,8,10].The combined course of IHD and AH is characterized by a more pronounced immune-inflammatory imbalance compared to isolated forms of cardiovascular pathology. This condition is associated with the formation of a specific immunopathological phenotype, including increased pro-inflammatory activity, impaired cellular immunity, and compensatory changes in humoral immune responses. However, despite the growing understanding of the immunological mechanisms involved, clinical practice still relies predominantly on hemodynamic and metabolic approaches to treatment, while the immune component of the disease remains largely under-addressed [1,3]. In this context, immunocorrective therapy represents a promising direction aimed at modulating systemic inflammation and restoring immune homeostasis. Experimental and clinical studies suggest that targeted correction of immune dysfunction may contribute to improved endothelial function, stabilization of atherosclerotic plaques, and reduction of inflammatory activity. Nevertheless, the clinical effectiveness of immunocorrective interventions in patients with IHD associated with AH remains insufficiently investigated, particularly in relation to their impact on both immunological parameters and clinical outcomes [4,12,13].Importantly, there is a lack of integrated approaches that combine clinical, functional, and immunological indicators into a unified system for assessing disease severity and treatment effectiveness. The absence of standardized criteria for evaluating immune-inflammatory imbalance limits the ability to personalize therapy and objectively monitor treatment response. In particular, the prognostic and clinical value of combined immunological markers, including cytokine profiles and T-cell subpopulations, has not been fully elucidated in this patient population [5,6].Purpose of the study. To evaluate the impact of immunocorrective therapy on systemic immune-inflammatory imbalance in patients with ischemic heart disease associated with arterial hypertension and to substantiate the feasibility of a differentiated therapeutic approach based on clinical and immunological parameters.
2. Materials and Methods
- The study included 120 patients aged 35 to 75 years with verified ischemic heart disease (IHD) associated with arterial hypertension (AH), who were observed at the Bukhara Regional Cardiology Dispensary.The diagnosis of IHD was established based on clinical symptoms, electrocardiography (ECG), and echocardiographic findings, as well as functional classification according to the Canadian Cardiovascular Society (CCS). The severity of chronic heart failure was assessed using the New York Heart Association (NYHA) classification. Arterial hypertension was diagnosed according to current clinical guidelines based on repeated blood pressure measurements.All patients underwent a comprehensive clinical, laboratory, and instrumental examination, including assessment of clinical status, hemodynamic parameters, and functional condition of the cardiovascular system.Laboratory and immunological assessment was performed using peripheral blood and serum samples. The cellular component of the immune system was evaluated by determining T-lymphocyte subpopulations, including CD3⁺ (total T-lymphocytes), CD4⁺ (T-helper cells), CD8⁺ (cytotoxic T-lymphocytes), and calculation of the CD4/CD8 ratio. The humoral immune response was assessed by measuring immunoglobulin G (IgG) levels.Markers of systemic inflammation were determined, including high-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), and interferon-gamma (IFN-γ). In addition, NT-proBNP levels were measured as a marker of neurohumoral activation and heart failure severity.Patients were divided into two groups depending on the treatment strategy. The first group received standard therapy in accordance with current clinical guidelines for the management of IHD and AH. The second group, in addition to standard therapy, received immunocorrective therapy aimed at modulating systemic immune-inflammatory processes.The effectiveness of therapy was evaluated based on changes in clinical, functional, and immunological parameters. Clinical effectiveness was assessed by reduction in the frequency of angina attacks, improvement in functional class according to CCS and NYHA, and increased exercise tolerance. Functional assessment included evaluation of hemodynamic and echocardiographic parameters.Immunological effectiveness was assessed by changes in T-cell subpopulations (CD3⁺, CD4⁺, CD8⁺), normalization of the CD4/CD8 ratio, reduction in pro-inflammatory cytokines (IL-6 and hs-CRP), and changes in IFN-γ and IgG levels.To obtain an integrated assessment of systemic immune-inflammatory imbalance, an integral immune-inflammatory risk scale (IICRS) was applied, based on a combination of clinical, functional, laboratory, and immunological indicators. This scale allowed quantitative evaluation of the severity of immune-inflammatory disturbances and was used to assess the effectiveness of immunocorrective therapy.Statistical analysis was performed using standard methods of medical statistics. Quantitative data were expressed as mean values (M±m). Differences between groups were considered statistically significant at p<0.05.
3. Results and Discussion
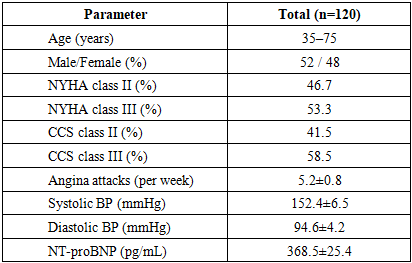
- The analysis of clinical, functional, and immunological data demonstrated that patients with ischemic heart disease associated with arterial hypertension were characterized by a pronounced systemic immune-inflammatory imbalance, which significantly contributed to disease progression and clinical severity.Baseline clinical and functional characteristics of the examined patients are presented in Table 1.
|
|
|
4. Conclusions
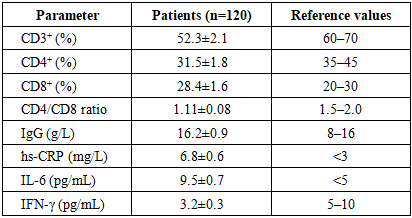
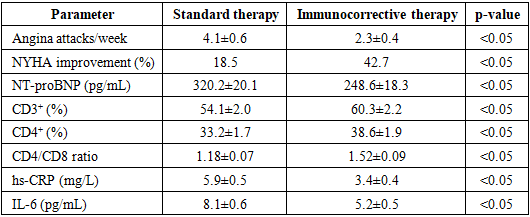
- Patients with ischemic heart disease associated with arterial hypertension are characterized by a pronounced systemic immune-inflammatory imbalance, manifested by elevated levels of pro-inflammatory markers (hs-CRP, IL-6), reduced IFN-γ, decreased CD3⁺ and CD4⁺ T-lymphocytes, and a lowered CD4/CD8 ratio, along with compensatory activation of humoral immunity (increased IgG levels).The severity of immune-inflammatory disturbances is closely associated with clinical and functional status, including the frequency of angina attacks, NYHA functional class, and NT-proBNP levels, indicating a significant role of immune dysregulation in the progression of cardiovascular pathology.Standard therapy provides limited correction of immune-inflammatory imbalance and is primarily associated with moderate clinical improvement, without significant normalization of immunological parameters.The inclusion of immunocorrective therapy in the treatment regimen leads to significantly greater clinical and laboratory improvements, including reduction in angina frequency, improvement in functional class, decreased NT-proBNP levels, and increased exercise tolerance.Immunocorrective therapy contributes to the restoration of cellular immunity, as evidenced by increased CD3⁺ and CD4⁺ T-lymphocyte levels and normalization of the CD4/CD8 ratio, as well as suppression of systemic inflammation through a significant reduction in hs-CRP and IL-6 levels.The use of an integral immune-inflammatory risk scale (IICRS) allows objective assessment of the severity of immune-inflammatory imbalance and provides a useful tool for evaluating treatment effectiveness and guiding personalized therapeutic strategies.