-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 2071-2075
doi:10.5923/j.ajmms.20261604.103
Received: Mar. 25, 2026; Accepted: Apr. 22, 2026; Published: Apr. 25, 2026

Genetic Predictors of Endothelial Dysfunction in Arterial Hypertension and Renal Dysfunction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdizova D. R.1, Boboev Q. T.1, Jarilkasynova G. J.2
1Bukhara State Medical Institute, Bukhara, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Hematology, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study evaluated the association of the NOS3 gene T-786C polymorphism with arterial hypertension (AH) and renal dysfunction. Genotypes were analyzed in patients with AH, including those with renal impairment, and compared to a control group. The mutant C allele was associated with a 3.1-fold increased risk of renal dysfunction (OR = 3.1; 95% CI 1.73–5.42) and a 2.1-fold higher likelihood of developing AH (OR = 2.1; 95% CI 1.18–3.74) compared to controls. These results indicate that the C allele of the NOS3 T-786C polymorphism may serve as a genetic marker for early identification of individuals at risk for hypertension and hypertension-related renal damage.
Keywords: Arterial hypertension, Renal dysfunction, NOS3 gene, T-786C polymorphism, Genotype, Allele, Genetic marker
Cite this paper: Adizova D. R., Boboev Q. T., Jarilkasynova G. J., Genetic Predictors of Endothelial Dysfunction in Arterial Hypertension and Renal Dysfunction, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 2071-2075. doi: 10.5923/j.ajmms.20261604.103.
1. Introduction
- Arterial hypertension (AH) remains a pressing issue in modern medicine due to its high prevalence, frequent complications, significant impact on patients’ quality of life, and substantial economic burden on healthcare systems. It is projected that by 2030, the global number of individuals with AH will exceed 1.5 billion. AH is a multifactorial disease, the development of which is influenced by numerous risk factors acting through complex pathogenetic mechanisms. Moreover, AH is a major risk factor for cardiovascular and renal damage [4,8,12]. The endothelial nitric oxide synthase (eNOS) plays a central role in human physiology by ensuring the production of nitric oxide (NO). NO regulates vascular tone and exerts anti-inflammatory and antithrombotic effects. Insufficient NO production leads to significant disturbances in cardiovascular and renal hemodynamics. Consequently, endothelial dysfunction develops, characterized by reduced NO biosynthesis or diminished biological activity, which contributes to the pathogenesis of conditions such as arterial hypertension, atherosclerosis, cardiomyopathies, as well as ischemic and sclerotic kidney damage [2,6,10]. These disturbances lead to the development of renal dysfunction, impaired perfusion of the heart and kidneys, activation of neurohormonal systems (renin–angiotensin–aldosterone system, sympathetic nervous system), increased oxidative stress, and endothelial dysfunction, thereby forming a mutually reinforcing pathological cycle.A substantial body of literature has focused on the role of reduced endothelial nitric oxide synthase activity in decreasing NO biosynthesis and contributing to the formation of this pathological cycle in arterial hypertension and associated renal dysfunction. Several studies have also investigated genetic predisposition, although the findings across different populations remain inconsistent [1,5,7].For instance, Uwabo et al. examined the association of the 27-bp VNTR polymorphism of the eNOS gene with arterial hypertension in a population north of Tokyo. The authors found that the frequency of the a allele was significantly higher in the hypertensive group compared to the control group. Logistic regression analysis indicated that the a allele could be considered a genetic marker of arterial hypertension in Japanese patients [11].The results of several studies demonstrate that genetic polymorphisms in exon 7 and the promoter region of the eNOS gene, as well as elevated levels of certain plasma biomarkers, are associated with the development of arterial hypertension. Endothelial dysfunction is considered a key vascular mechanism underlying this pathological process. Data on genetic predisposition are of significant value for identifying at-risk populations and can be utilized in the development of molecularly targeted preventive and therapeutic strategies for arterial hypertension [9,13].In the Uzbek population, the significance of the T-786C polymorphism of the NOS3 gene in the development of renal dysfunction in patients with chronic heart failure has been investigated. It has been shown that this polymorphism negatively affects NOS3 gene activity in patients with renal dysfunction, leading to reduced nitric oxide synthesis and, consequently, impaired vascular regulation [3].Objective: To investigate the genetic significance of the T-786C polymorphism of the NOS3 gene in the etiological interplay of arterial hypertension and renal dysfunction in the Uzbek population.
2. Materials and Methods
- This study was conducted at a multidisciplinary clinic of the Bukhara State Medical Institute among patients with arterial hypertension receiving both outpatient and inpatient care. A total of 200 individuals were included and divided into two main groups and one control group. The main group consisted of 160 patients with arterial hypertension, with a mean age of 62.69 ± 5.4 years. This group was further subdivided into two subgroups: patients with renal dysfunction and those without renal dysfunction. The diagnosis of arterial hypertension and renal dysfunction was carried out in accordance with the clinical guidelines of the European Society of Cardiology (ESC) and the KDIGO (Kidney Disease: Improving Global Outcomes) criteria (2018, 2021, 2024).All patients initially underwent an assessment of complaints, medical and life history, and general clinical status. Standard laboratory tests were performed, including complete blood count, urinalysis, biochemical parameters (creatinine, urea, lipid profile, glucose), and hemostasis system indicators.Molecular-genetic studies were conducted at the Department of Molecular Medicine and Cell Technologies of the Republican Specialized Scientific and Practical Medical Center of Hematology. DNA was extracted from peripheral blood using the “AmpliPrime RIBO-prep” kit (AmpliSens, Russia). The concentration of the extracted DNA was measured using a NanoDrop 2000 spectrophotometer (NanoDrop Technologies, USA) at a wavelength of A260/280 nm. The purity of all DNA samples, assessed by the A260/280 ratio, ranged from 1.7 to 1.8.To determine the T-786C polymorphism of the NOS3 gene, commercial test kits from Litekh (Moscow) were used. Polymerase chain reaction (PCR) was performed using a Rotor-Gene Q thermocycler (QIAGEN, Germany) according to the amplification program.Statistical analysis included evaluation of genotype distribution conformity to Hardy–Weinberg equilibrium using the “GenePop” program (“Genetics of Population”) (http://wbiomed.curtin.edu.au/genepop). Calculations were performed using the software package OpenEpi 2009, Version 9.2.
3. Results
- Analysis of the genotype frequencies of the T-786C polymorphism of the NOS3 gene (T/T, T/C, and C/C) among the study participants showed the following distribution: in the first main group (patients with renal dysfunction), the genotypes were distributed as 32.5% (T/T), 27.5% (T/C), and 40.0% (C/C).In the second group (patients without renal dysfunction), the genotype distribution was 40.0% (T/T), 31.3% (T/C), and 28.7% (C/C). In the control group, the distribution was 55.0% (T/T), 35.0% (T/C), and 10.0% (C/C).The allele frequencies in patients with renal dysfunction were: favorable T allele — 46.3%, and unfavorable C allele — 53.8%. In patients without renal dysfunction, the T allele frequency was 55.6% and the C allele frequency was 44.4%. In the control group, these values were 72.5% and 27.5%, respectively (Figure 1).
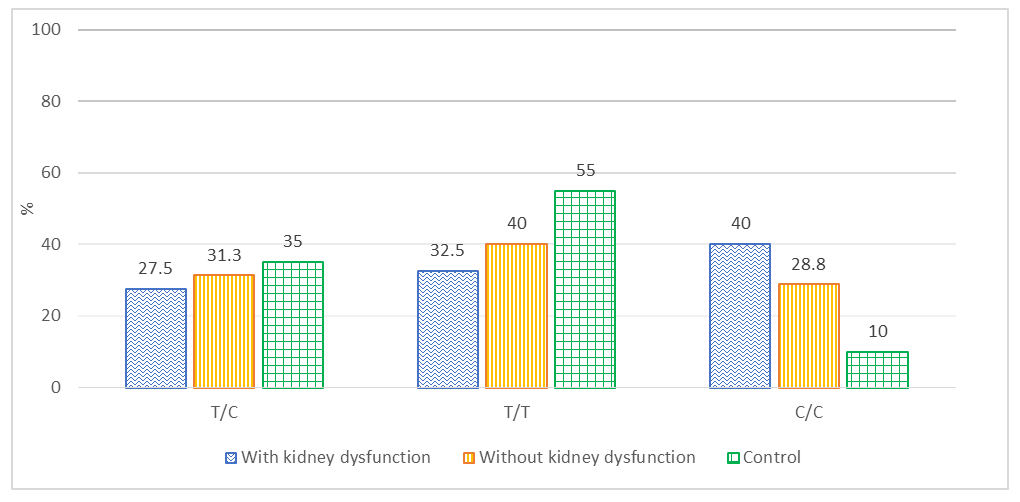 | Figure 1. Comparative analysis of the genotype distribution of the NOS3 T-786C polymorphism among the study groups (%) |
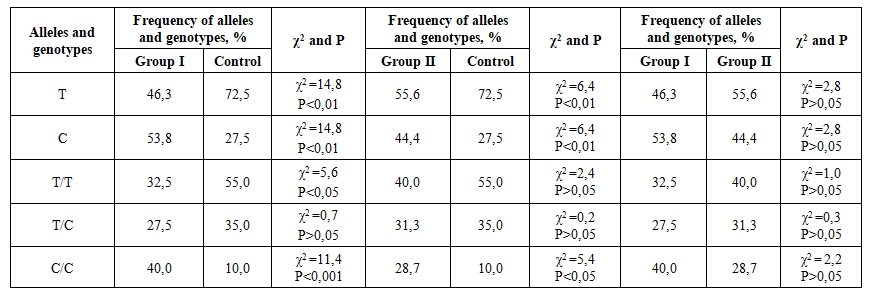 | Table 1. Comparative analysis of the frequency of alleles and genotypes of the T-786C polymorphism of the NOS3 gene in the groups |
4. Conclusions
- The presence of the mutant homozygous C/C genotype in the first main group, compared to the control group, is associated with a fourfold increase in the risk of renal dysfunction and a sixfold increase in the odds of disease development (RR = 4.0; 95% CI 2.61–6.14; OR = 6.0; 95% CI 2.12–16.96). The higher frequency of this genotype in patients with arterial hypertension, compared to controls, significantly increases the risk of developing arterial hypertension by 2.9-fold and the odds of disease by 3.6-fold (RR = 2.9; 95% CI 1.85–4.47; OR = 3.6; 95% CI 1.22–10.8). The presence of the mutant C allele in the first main group, compared to the control group, is associated with a 3.1-fold increase in the likelihood of renal dysfunction, and in patients with arterial hypertension, with a 2.1-fold increase in the risk of developing hypertension (OR = 3.1; 95% CI 1.73–5.42 and OR = 2.1; 95% CI 1.18–3.74, respectively).These findings suggest that genetic analysis of the NOS3 T-786C polymorphism may serve as a potential screening tool for identifying hereditary predisposition to arterial hypertension and associated renal dysfunction.