-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1599-1604
doi:10.5923/j.ajmms.20261604.10
Received: Mar. 2, 2026; Accepted: Mar. 29, 2026; Published: Apr. 1, 2026

The Role of Matrix Metalloproteinases and Pro-Inflammatory Cytokines in the Pathogenesis of Dorsalgia in Modic-Type Spondylodiscitis and the Effectiveness of Pathogenetic Therapy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdambaev Z. I.1, Mirjuraev E. M.2, Samiev A. S.3, Ergashev G. B.4
1Urgench State Medical Institute, Urgench, Uzbekistan
2Center for the Development of Professional Qualifications of Medical Workers, Tashkent, Uzbekistan
3Samarkand State Medical University, Samarkand, Uzbekistan
4Central District Hospital of Narpay District, Neurology Department, Samarkand, Uzbekistan
Correspondence to: Adambaev Z. I., Urgench State Medical Institute, Urgench, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article highlights current aspects of the etiology, pathogenesis, and treatment of dorsalgia associated with Modic-type spondylodiscitis. Data on the infectious (Propionibacterium acnes) and autoimmune origins of bone marrow changes are analyzed, along with the role of MMP-3 and MMP-9, their TIMP-1, and pro-inflammatory cytokines (IL-1β, TNF-α, IL-6) in the development of inflammation and intervertebral disc degradation. A review of clinical manifestations, standardized assessment scales, and treatment approaches, including antibiotic and anti-inflammatory therapy, is presented. Special attention is given to the results of the authors’ own study evaluating the effectiveness of comprehensive conservative treatment in 100 patients with aseptic Modic type I spondylodiscitis. It was demonstrated that the inclusion of paravertebral blocks with hydrocortisone and ultrasound therapy (phonophoresis) with “Cariflex” gel in the treatment regimen resulted in a more pronounced reduction in pro-inflammatory cytokine levels and extracellular matrix degradation markers compared with standard therapy. These findings indicate more effective modulation of the inflammatory process and improvement of bone tissue metabolism.
Keywords: Dorsalgia, Spondylodiscitis, Modic changes, Biomarkers, MMP-3, MMP-9, TIMP-1, Pro-inflammatory cytokines, Paravertebral blocks, Phonophoresis
Cite this paper: Adambaev Z. I., Mirjuraev E. M., Samiev A. S., Ergashev G. B., The Role of Matrix Metalloproteinases and Pro-Inflammatory Cytokines in the Pathogenesis of Dorsalgia in Modic-Type Spondylodiscitis and the Effectiveness of Pathogenetic Therapy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1599-1604. doi: 10.5923/j.ajmms.20261604.10.
1. Introduction
- The idea of dorsalgia with the type of spondylodiscitis is one of the most disputable problems in the modern vertebrology and neurology as verified by various reviews and primary studies [1,5,43]. Modic changes were initially defined in 1988 as being MRI-detected changes in bone marrow around vertebral endplates and are common in the context of degenerative spinal disease, including that of spondyloarthrosis affecting facet joints, intervertebral discs, and its surrounding bone. According to the epidemiological data, the shifts are observed among 6-25 per cent of patients with chronic back pain and are associated with increased pain intensity and decreased quality of life indicators [18,27,34]. Since the nonspecific back pain affects between 50 and 80 percent of adults and causes significant economic losses due to disability, it is evident that the subject has clinical and socioeconomic significance [1,5,44].Recent theory approaches of pathogenesis emphasize a mixed infectious-immune pathogenesis, especially in type 1 lesions of Modic type. Potential research indicates that Propionibacterium acnes has been detected in 40-80 percent of intervertebral discs of patients with the presence of the Modic type 1 changes, being higher than the control groups [7,13,16]. Experimental rabbit models also show that disc inoculation with P. acnes has the opportunity to cause bone marrow edema which mimic a change of Modic changes within 6-12 months [41]. The mechanism by which low-virulence disc infection triggers local inflammation is mechanistically proposed to involve the release of IL-1-b, TNF-a and IL-6, which is further augmented by secondary immune response and production of vasogenic edema [15,37]. In line with this hypothesis, Dudli et al. (2018) suggested that Modic type 1 occurs against an infected disc co-existed with a pro-inflammatory bone marrow microenvironment [15], other studies report an increase in Cytokine activity and autoantibody activity in the sufferers [32]. Risk may additionally be genetic susceptibility modified through the immune-related polymorphisms [24,26].MRI is still the mainstay of diagnostic imaging and phenotyping. T1 hypointensity and T2/STIR hyperintensity that are typical of active edema and inflammation characterize modic type 1 and is the best associated with clinically relevant pain [20,21,35]. Modic type 2 is a manifestation of fatty marrow replacement, and is generally more stable, whereas type 3 is associated with the sclerosis, and least often does it relate to pain [13,35]. Symptoms are heterogeneous and vary according to spinal level and neural involvement and include mechanical local pain, referred pain, radiculopathy, or neurogenic claudication and in severe cases, sensory and motor deficit [8,23]. The severity of the symptoms and pain treatment response are well quantified using standardized assessment tools like Visual Analogue Scale (VAS) of pain and Oswestry Disability Index (ODI) of disability, as well as the SF-36 and EQ-5D instruments to indicate a pronounced impairment of quality of life in this group of patients [8,43,44].Alongside imaging, biomarker profiling is also an area that is being studied to quantitatively measure disease activity. Though the levels of C-reactive protein (CRP) tend to be normal or with a low-grade of inflammation [2,11], IL-6 is considered as one of the main mediators of pain sensitization and tissue remodelling [11,37]. The involvement of matrix metalloproteinases (especially, MMP -3 and MMP -9) in the breakdown of extracellular matrix in disc and adjacent structures; a disproportion between them and their inhibitor tissue inhibitor of metalloproteinases -1 (TIMP -1) may support progressive destruction; these parameters have been suggested as diagnostic and prognostic measures of active degenerativeinflammatory processes [2,5,7,10,12,13,30].Therapy is a divisive matter. Certain trials suggest that an extended course of antibiotic therapy (e.g. amoxicillin -clavulanate) is superior to placebo in selected patients [8-10], but later meta-analytic studies indicate that the effect is not consistent [12]. The non-steroid anti-inflammatory drugs only serve as first-line treatment and may be effective with adjunctive treatment, but cannot be used long-term due to their adverse effects [2,11]. New pathogenetic methods, such as regulation of the microbiome, have also been proposed [19]. Surgical intervention is used when there is deterioration or worsening of the neurological condition; Modic type 1 changes were reported to have a poorer postoperative prognosis [29]. Prognosis is inconsistent; Modic type 1 has been established as an independent determinant of worse outcome to conservative therapy, especially in patients with a history of pain lasting longer than 12 months, multilevel disease, CRP 2. 10mg/L, and resistance to NSAIDs [14,16], though an early, pathogenetically targeted treatment can stabilise remission in 6070 per cent of cases [8,10].It is against this background that the objective of the current research was to assess the efficacy of conservative therapy in the case of aseptic Modic type 1 spondylodiscitis in the presence of para vertebral hydrocortisone blocks coupled with ultrasound therapy (phonophoresis) using Cariflex gel.
2. Materials and Methods
- A prospective comparative clinical study was conducted in the Neurology Department of the Central District Hospital of Narpay District (CRH Narpay) and included 100 patients diagnosed with aseptic spondylodiscitis (ASD) corresponding to Modic type I changes in the lumbosacral spine. The cohort comprised 65 men and 35 women. The mean age of the total sample was 50.2±2.4 years; mean age in men was 48.1±2.5 years and in women 53.3±2.3 years. The diagnosis and phenotyping of ASD according to Modic type I were established by magnetic resonance imaging (MRI) of the lumbar spine.
|
|
3. Results
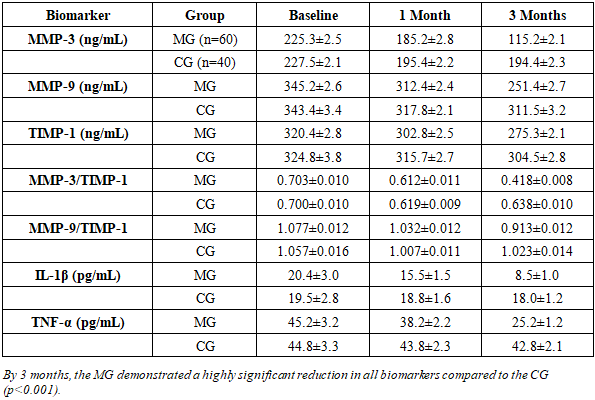
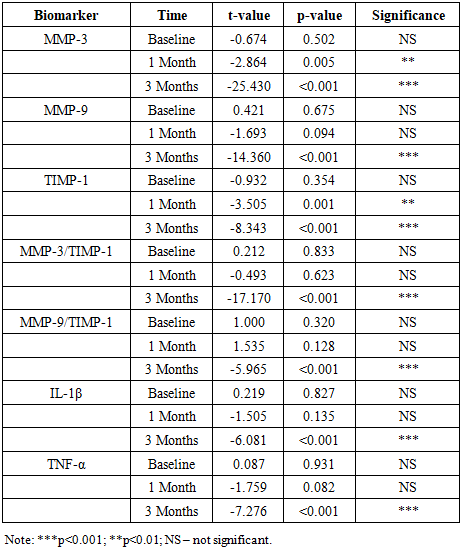
- At baseline, all patients presented with Modic type I aseptic spondylodiscitis confirmed by MRI. Clinically, the dominant symptom was deep, aching or pulsating lumbosacral pain aggravated by physical load and frequently intensified at night. Radicular pain radiating to the lower extremities was observed in 79% of patients and was commonly associated with paresthesia. Morning stiffness lasting more than 30 minutes was reported by 60% of patients, and severe limitation of spinal range of motion was documented in 85%.Neurological examination revealed radicular syndromes in 51% of patients. Decreased tendon reflexes and sensory disturbances in the corresponding dermatomes were observed in 55%, while objective muscle weakness was present in 11%. MRI additionally demonstrated disc herniation in 90% of cases, spondylolisthesis in 20%, and vertebral osteoporosis in 30%, predominantly among women older than 50 years.Baseline comparison showed that the MG and CG were statistically comparable across all biomarker levels (p>0.05), allowing objective evaluation of treatment effects.
|
|
4. Conclusions
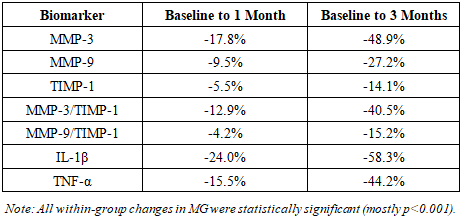
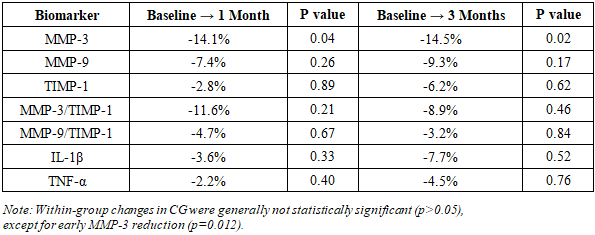
- Aseptic type I Modic spondylodiscitis is characterized by eminent clinical presentation, which includes persistent lumbosacral and radicular pain, loss of functionality, and neurological impairments usually accompanied with disc herniation and other degenerative changes. The disorder is biochemically linked with increased amount of MMP-3, MMP-9, IL-1, and TNF-A and the disproportion of MMP/TIMF ratios, which reflects active inflammatory and matrix-destructive actions.The treatment regime that was combined with the paravertebral hydrocortisone blocks and ultrasound phonophoresis using a Cariflex gel led to a statistically significant decrease in all the biomarkers studied after three months of treatment compared to the usual therapy. Significant reductions in MMP-3, MMP-9, pro-inflammatory cytokines as well as normalization of MMP/TIMP ratios indicate successful inhibition of inflammation and some restoration of extracellular matrix balance.These findings support the idea of the conceptualization of the Modic type I changes as an active inflammatory-degenerative process and prove that pathogenetically-oriented combination therapy has a better clinical and molecular outcome. There is a need to conduct further controlled studies that would validate the use of biomarkers in the management of this group of patients.