-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1586-1591
doi:10.5923/j.ajmms.20261604.08
Received: Feb. 28, 2026; Accepted: Mar. 15, 2026; Published: Apr. 1, 2026

Modern Treatment Methods of Hip Osteoarthritis in Patients After COVID-19 and Their Long-Term Outcomes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShodikulova Gulandom Zikriyayevna, Khasanov Oybek Gafurovich, Kiyamov Azizbek Utkirovich
Samarkand State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

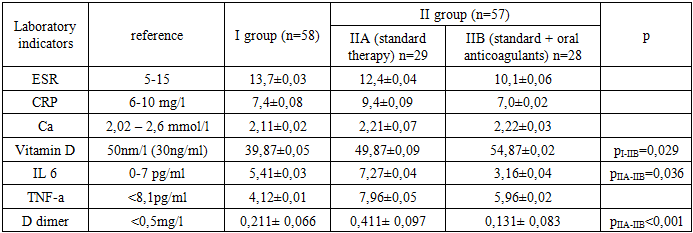
The study is devoted to comparing the clinical, laboratory, and instrumental features of hip osteoarthritis (HOA) in patients who have recovered from COVID-19 infection with those of idiopathic osteoarthritis (IOA). During 2023–2024, 119 patients were examined at medical institutions in Samarkand: 62 with idiopathic OA and 57 with post-COVID OA. Patients in the second group received standard therapy combined with an anticoagulant (rivaroxaban 20 mg/day). Non-pharmacological measures included physical activity, body weight control, and physiotherapy, while pharmacological treatment consisted of chondroprotectors, nonsteroidal anti-inflammatory drugs (NSAIDs), steroids, calcium, and vitamin D. In the group receiving anticoagulant therapy, reduction in pain (7.1%), crepitus (7.1%, pI-IIB=0.043), limping (3.5%, p=0.041), and muscle spasms (p=0.041) was observed. Laboratory analysis showed decreased levels of inflammatory markers (ESR, C-reactive protein, IL-6, TNF-α) and a reduction in D-dimer concentration to 0.131 mg/L (p<0.001), indicating a lower risk of thrombosis and improved microcirculation under the influence of anticoagulant therapy. Thus, anticoagulant therapy in post-COVID osteoarthritis represents an important component of comprehensive treatment, effectively reducing inflammation and thrombosis, improving microcirculation, and restoring musculoskeletal function. These findings provide a scientific basis for incorporating anticoagulants into individualized rehabilitation and pharmacotherapy strategies for patients with post-COVID osteoarthritis.
Keywords: Hip osteoarthritis, COVID-19, Anticoagulant therapy, Rivaroxaban, Inflammatory markers, Microcirculation, Rehabilitation
Cite this paper: Shodikulova Gulandom Zikriyayevna, Khasanov Oybek Gafurovich, Kiyamov Azizbek Utkirovich, Modern Treatment Methods of Hip Osteoarthritis in Patients After COVID-19 and Their Long-Term Outcomes, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1586-1591. doi: 10.5923/j.ajmms.20261604.08.
1. Introduction
- Hip osteoarthritis (HOA) is one of the most prevalent chronic degenerative diseases of the musculoskeletal system and represents a major cause of pain, disability, and reduced quality of life worldwide. According to the Global Burden of Disease study, osteoarthritis affects more than 500 million people globally, with hip involvement accounting for a significant proportion of cases and contributing substantially to years lived with disability. The prevalence of hip osteoarthritis increases with age and is expected to rise further due to population aging, increasing obesity rates, and decreased physical activity levels [1,2,3].In recent years, the COVID-19 pandemic has introduced new challenges in understanding the pathogenesis and clinical course of musculoskeletal diseases. Numerous international studies have demonstrated that SARS-CoV-2 infection is associated with systemic inflammation, endothelial dysfunction, and hypercoagulability, which may significantly affect joint tissues and periarticular microcirculation. Persistent post-COVID syndrome has been linked to chronic inflammatory responses and microvascular damage, potentially accelerating degenerative processes in articular cartilage and subchondral bone [4,5].Several studies from Europe, the United States, and China have reported that patients recovering from COVID-19 frequently experience musculoskeletal complications, including arthralgia, myalgia, and exacerbation of pre-existing osteoarthritis. Elevated levels of inflammatory cytokines such as IL-6 and TNF-α, as well as increased D-dimer levels, have been associated with impaired microcirculation and increased thrombotic risk, which may worsen joint perfusion and contribute to disease progression. These findings highlight the potential role of anticoagulant therapy not only in preventing thrombotic events but also in improving tissue perfusion and reducing inflammation in patients with post-COVID osteoarthritis [6,7,8].In Uzbekistan, osteoarthritis remains a significant public health concern, particularly among the aging population. Epidemiological observations indicate a steady increase in the incidence of degenerative joint diseases, including hip osteoarthritis, over the past decade. In addition, the high burden of COVID-19 infection in the region has led to a growing number of patients presenting with post-COVID complications, including musculoskeletal disorders. Clinical observations in Samarkand and other regions of Uzbekistan suggest that patients with a history of COVID-19 often demonstrate a more severe clinical course of osteoarthritis, characterized by increased pain, functional limitations, and laboratory signs of systemic inflammation [9,10,11].Given the growing number of patients with post-COVID osteoarthritis and the potential role of microcirculatory disturbances and hypercoagulability in its pathogenesis, the search for effective therapeutic strategies is of great clinical importance [12,13]. In particular, the use of anticoagulant therapy as part of complex treatment may represent a promising approach to improving clinical outcomes in this patient population.The aim of this study was to compare the clinical, laboratory, and instrumental parameters of patients with hip osteoarthritis after COVID-19 infection with those of idiopathic osteoarthritis, as well as to evaluate the effectiveness of treatment using an anticoagulant (rivaroxaban).
2. Materials and Methods
- The scientific study was conducted in 2023–2024 on the basis of the Samarkand City Medical Association and the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Center of Traumatology and Orthopedics. The study included 119 patients, in particular, 62 (52.1%) of them - 21 men (33.9%) and 41 women (66.1%) - were diagnosed with idiopathic osteoarthritis (main group) and were with aged from 20 to 66 years (48.01±1.4). 57 (47.9%) patients aged from 19 to 55 years (42.17±1.28) with hip joint osteoarthritis after COVID-19 infection (comparative group) - 24 (42.1%) men and 33 (57.9%) women - were included in the study within the framework of prospective analysis from the Samarkand City Medical Association and the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Center of Traumatology and Orthopedics. Both groups of patients received traditional treatment methods. The control group consisted of 78 practically healthy individuals. Additionally, the patients of the second study group were divided into two subgroups due to the addition of supplementary drugs to the traditional treatment regimen: subgroup IIA consisted of 28 patients who received only standard treatment methods; subgroup IIB patients (n=29) received, in addition to standard therapy, oral anticoagulant medication Rivaroxaban 20 mg, 1 tablet once daily for a long period (at least 6 months) under control of blood coagulation parameters. In the subgroups, studies were conducted based on the analysis of clinical and laboratory results during one year. When patients in the study were treated with non-drug and drug therapy, the long-expected outcomes were as follows. Non-drug therapy: The treatment method was chosen based on mutual decision between the patient and the specialist. Weight reduction: normalization of body weight is recommended for patients with knee and hip joint osteoarthritis suffering from overweight or obesity. For patients with excessive body weight (BMI >25 kg/m²), it is recommended to lose at least 5% of their weight within 6 months or at least 10% within 1 year. The following exercises are recommended: aerobic, strength or resistance, flexibility and stretching exercises, preferably performed in water. Orthopedic recommendations included choosing shoes that are comfortable, with good cushioning, large enough to ensure the comfortable position of the toes, and without high heels. Physiotherapeutic treatment methods was represented by balneotherapy (sulfur and radon baths). Drug therapy: Basic chondroprotectors: Chondroitin sulfate 500 mg twice a day, Glucosamine sulfate 750 or 1500 mg twice a day, Combined preparations (Chondroitin and Glucosamine) from 250 to 500 mg 1 to 3 times a day, Diacerein 50 mg twice a day - these medicines were used for a long time (at least 6 months) according to the indicated dosages. Anti-inflammatory steroid drugs - according to indications (in case of synovitis or severe pain): Betamethasone dipropionate/sodium phosphate 7 mg/ml intramuscularly or intra-articularly according to the scheme; Triamcinolone acetonide 40 mg/ml intramuscularly or intra-articularly according to the scheme. Non-steroidal anti-inflammatory drugs: in cases where joint inflammation signs were pronounced and pain was severe, treatment began with injectable forms of drugs: Diclofenac 3 ml amp. 25 mg/ml intramuscularly once a day, Ketoprofen 2 ml 50 mg intramuscularly once a day, Tenoxicam 20 mg lyophilized powder and solvent vial intramuscularly or intravenously once a day, Lornoxicam 8 mg vial intravenously or intramuscularly, Meloxicam 15 mg/1.5 ml ampule intramuscularly once a day - in chronic course with constant pain, NSAIDs were prescribed in outpatient conditions. Calcium-containing drugs: Calcemin, calcium gluconate, and combined forms with vitamin D3 (Calcium D3) were used. Aqua D3 10,000 IU once daily for 1 month, Vitamin D3 10,000 IU tablet once daily for 1 month were used in the same dosage.Statistical analysis was performed with IBM SPSS 27 by using nonparametrical criterias and exact Fisher’s/Pearson's chi-squared test.
3. Obtained Results
- In the study, clinical signs in Group I and Group II, as well as long-term treatment results between patients treated with standard and additional anticoagulant therapy, were compared. Based on the results, pain syndrome - in Group I was observed in 17.7% of patients. In Group IIA (standard treatment), pain was noted in 17.5% of patients; in Group IIB (standard + oral anticoagulants), pain was observed in 6.9% of patients. No statistical difference was observed, however the lower incidence of pain in Group IIB, where anticoagulants were prescribed, might be associated with the improvement of microcirculation in bone and joint tissues and the reduction of inflammation by these drugs. Crepitus (crackling) - in Group I: 18 (29%), in Group IIA: (25%), in Group IIB: 6.9%. The decrease in crepitus in Group IIB (pI-IIB=0.043), where anticoagulants were used, indicates a possible reduction in degenerative processes in the joints and the restoration of joint lubrication (synovial fluid) volume. Limping was observed in 21 (33.9%) patients of Ist, 10 (35.7%) - IIA and 1 (3.4%) - IIB groups. In Group IIB, the incidence of limping decreased almost tenfold (pI-IIB=0.022, pIIA-IIB=0.021). This indicates that anticoagulants improve microcirculation, accelerate recovery of muscles and ligaments, and enhance motor functions. The frequency of muscle spasms was as follows: in Group I - 9 (14.5%) patients, in Group IIA - 3 (10.7%), and in Group IIB - 1 (3.4%). Despite the apparent reduction in the frequency of spasms in Group IIB, no statistically significant differences were found between the groups. Nevertheless, the observed trend is consistent with the hypothesis that anticoagulants, by improving peripheral circulation in the musculoskeletal system, may promote muscle relaxation.The reduction of thigh circumference (indicating muscle atrophy) was observed in 19 (30.6%) patients in Group I, 7 (25%) in Group IIA, and 3 (10.3%) in Group IIB. Although the incidence in Group IIB was approximately twofold lower, no statistically significant differences were found between the groups. Nonetheless, this numerical trend aligns with the possibility that anticoagulant therapy may contribute to positive changes in the musculoskeletal system. The incidence of such symptoms as difficulty in movement, which was reported in 17 (27.4%) of subjects in Group I, 7 (25%) - in Group IIA, and 6,9% - in Group IIB; and cramping in one or both legs, which occurred in 11.3% (Group I), 13.8% (Group IIA), and 3.57% (Group IIB); psycho-social disorders were present in 12.9% (Group I), 10.3% (Group IIA), and 3.57% (Group IIB) outlined the fact that Group IIB demonstrated a notably lower frequency across all measured parameters, statistical analysis did not reveal significant differences between the groups. The consistent numerical trends, however, suggest a potential positive correlation between anticoagulant therapy and the alleviation of these symptoms (Figure 1).
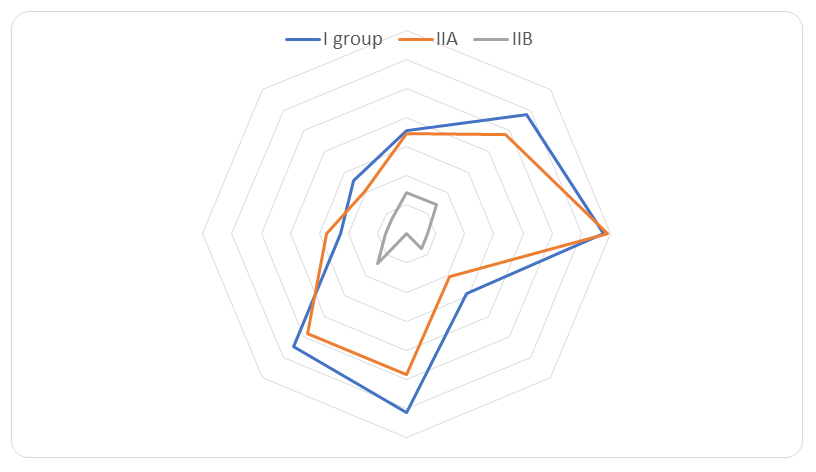 | Figure 1. Results of the influence of long-term treatment on the clinical symptoms of patients with hip joint osteoarthritis |
|
|
4. Conclusions
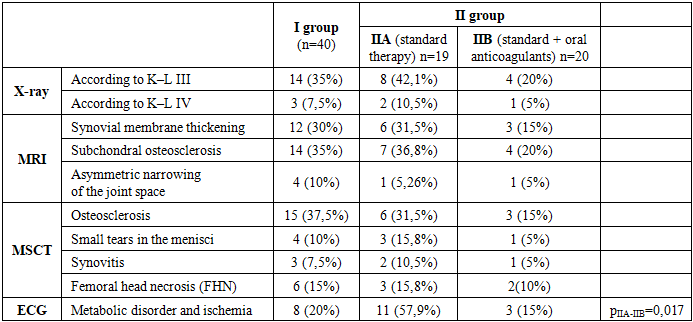
- Patients with a history of COVID-19 were observed to experience a more accelerated progression of hip osteoarthritis compared to those with the idiopathic form of the disease, characterized by a higher prevalence of pain, movement restriction, and inflammatory signs. The adjunctive use of anticoagulant therapy (rivaroxaban 20 mg/day) to standard treatment was associated with a significant reduction in pain syndrome, muscle spasms, and movement limitation. This clinical improvement corresponded with the normalization of key laboratory parameters-including IL-6, TNF-α, D-dimer, CRP, and ESR-indicative of diminished systemic inflammation and thrombotic risk. Instrumental assessments (X-ray, MRI, MSCT) further proved these findings, revealing reductions in subchondral osteosclerosis, synovitis, and ischemic alterations. These collective outcomes support the hypothesis that anticoagulants exert a positive effect on microcirculation and subsequent tissue regeneration. Integrating anticoagulation with established non-pharmacological interventions, such as physiotherapy, guided physical activity, and weight control, enhanced the overall efficacy of the comprehensive management strategy. In conclusion, anticoagulant therapy in the context of post-COVID-19 osteoarthritis appears to alleviate pain, improve mobility, mitigate inflammation, and promote structural recovery. This approach can be recommended as a pathogenetically grounded component in the management protocol for this condition.