-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1567-1570
doi:10.5923/j.ajmms.20261604.04
Received: Feb. 6, 2026; Accepted: Mar. 3, 2026; Published: Apr. 1, 2026

Analysis of Clinical Diagnostic Methods for Patients with Purulent-Necrotic Complications in the Maxillofacial Region in Systemic Vasculitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBoymuradov Sh. A., Hayitmurodov D. E., Djurayev J. A., Kurbanov Y. X., Sobirov E. E.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Systemic vasculitis comprises a group of severe chronic diseases characterized by immune-mediated inflammation of small and medium-sized blood vessels, affecting multiple organs and systems. The study was conducted from 2023 to 2026 at the departments of rheumatology, maxillofacial surgery, and otolaryngology of the multidisciplinary clinic of Tashkent State Medical University. In recent years, purulent-necrotic complications in the maxillofacial region have become increasingly common in patients with systemic vasculitis. This is caused by long-term immunosuppressive therapy, microcirculatory disorders, trophic tissue insufficiency, and the addition of secondary infections. Necrotic processes in the maxillofacial region are often masked by odontogenic infections, sinusitis, or purulent inflammation of soft tissues, leading to misdiagnosis and delayed treatment.
Keywords: Systemic vasculitis, Maxillofacial region, Purulent-necrotic complications, Surgical treatment, Necrectomy
Cite this paper: Boymuradov Sh. A., Hayitmurodov D. E., Djurayev J. A., Kurbanov Y. X., Sobirov E. E., Analysis of Clinical Diagnostic Methods for Patients with Purulent-Necrotic Complications in the Maxillofacial Region in Systemic Vasculitis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1567-1570. doi: 10.5923/j.ajmms.20261604.04.
1. Introduction
- Systemic vasculitis (SV) is a group of chronic multisystemic diseases affecting multiple organs, characterized by immune-mediated necrotic inflammation of small and medium-sized blood vessels. Their clinical manifestations are polymorphic and vary depending on the general condition of patients and the state of vascular and organ systems. In recent years, the increase in the incidence of systemic vasculitis and the complexity of its clinical manifestations have posed new diagnostic challenges for doctors, especially regarding the early detection of purulent-necrotic complications in the maxillofacial region [1,8].Purulent-necrotic processes in the maxillofacial region usually have severe consequences. They involve bone and soft tissues during the active phase of the disease, as well as odontogenic and sinusogenic components. Such changes significantly impact patients' pain sensitivity, oral and facial functions, as well as their psychological and social status. Furthermore, purulent-necrotic complications lead to chronic infections and bone and soft tissue defects that require surgical interventions [3,4,15].Information on the epidemiology of systemic vasculitis with purulent-necrotic complications in the maxillofacial region is limited in world literature. Foreign studies, such as those by Jennette et al. (2013) and Hellmich et al. (2018), have shown that purulent or necrotic processes in the maxillofacial region are detected in 25-35% of patients with types of systemic vasculitis, such as Wegener's granulomatosis and microscopic polyangiitis [2,5]. However, early diagnosis of such patients remains challenging in many clinical centers, as necrotic processes do not exhibit initial clinical signs or are mistaken for odontogenic inflammation. (2018), showed the detection of purulent or necrotic processes in the maxillofacial region in 25-35% of patients with TV types, such as Wegener's granulomatosis and microscopic polyangiitis [2,5].
2. Materials and Methods
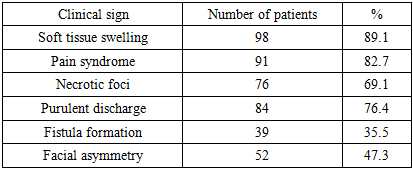
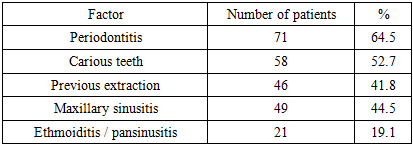
- The study was conducted from 2023 to 2026 at the departments of rheumatology, maxillofacial surgery, and otolaryngology of the multidisciplinary clinic of Tashkent State Medical University. The study included 110 patients with a confirmed diagnosis of systemic vasculitis based on clinical, laboratory, and instrumental criteria, who also had purulent-necrotic processes in the maxillofacial region. The patients' ages ranged from 18 to 68 years, with the majority being of working age. The inclusion criteria for the study were confirmed forms of systemic vasculitis (granulomatosis with polyangiitis, microscopic polyangiitis, eosinophilic granulomatosis with polyangiitis) and the presence of clinically and instrumentally confirmed necrotic changes in the maxillofacial region [7,14].The development of purulent-necrotic complications in the maxillofacial region associated with systemic vasculitis poses a significant risk to patients' health and surgical treatment outcomes. Therefore, the clinical diagnostic process for such patients is a crucial stage not only for identifying the pathological process but also for assessing its extent, determining the location and depth of purulent-necrotic changes, and establishing a strategy for surgical or conservative treatment. Clinical diagnosis requires an integrated approach, which includes a detailed medical history, general and local clinical examination, as well as an in-depth assessment of the dentofacial system and paranasal sinuses [6,10,13].Collecting a medical history is the first and most important step in identifying purulent-necrotic processes in the maxillofacial region in cases of systemic vasculitis. In addition to the patient's personal, family, and occupational history, the onset and progression of the disease are analyzed in detail. In our study, the collection of medical history included the following aspects:The onset of the disease was recorded, including when the patient first noticed symptoms and when initial signs (inflammation, pain, swelling) appeared, as well as how these changed over time. According to our study results, necrotic processes in the maxillofacial region often develop unnoticed during the first two years of the disease, with severity increasing as it progresses to a chronic stage. Previous infections were also noted. The patient's history of dental, sinus, and respiratory infections was analyzed in detail. This is particularly important for differential diagnosis between odontogenic inflammation and systemic vasculitis. It was observed that previous infections may predispose individuals to the development of necrotic processes.It was noted that patients had received long-term corticosteroid or cytostatic therapy, the use and dosage of immunosuppressive drugs, as well as a history of previous surgical interventions. This information is crucial for determining tissue regeneration capacity, inflammation intensity, and surgical rehabilitation strategy. The frequency of recurrence of purulent processes [12] was analyzed in the study, including the location of long-term complications and necrosis in patients. These data allow for a preliminary assessment of the effectiveness of surgical and conservative treatments. General health status and comorbidities were recorded. Chronic diseases, such as diabetes, hypertension, or immunodeficiency, were noted separately due to their potential to accelerate the development of necrotic processes and increase the risk of surgical complications. Through detailed history-taking, the clinical presentation of purulent-necrotic processes, tendencies towards chronic or acute progression, and individual patient characteristics were analyzed. This approach enhanced the possibility of developing individualized diagnostic and treatment strategies for patients. Clinical diagnostic results revealed that purulent-necrotic processes in the maxillofacial region associated with systemic vasculitis are often inconspicuous in the initial stages and can be confused with odontogenic or other local infections. Therefore, limiting oneself to symptomatic examinations is insufficient. Clinical diagnosis requires a comprehensive approach:detailed medical history,general and local clinical examination,assessment of lymph nodes and soft tissues,examination of the dentofacial system and paranasal sinuses.This approach allows for determining the localization and depth of necrotic processes in patients, the necessity for surgical intervention, and the effectiveness of conservative therapy. Furthermore, when clinical diagnostic results are combined with laboratory and instrumental studies, it significantly enhances the effectiveness of early detection and treatment of purulent-necrotic complications in the maxillofacial region. In the majority of patients, purulent-necrotic processes in the maxillofacial area manifested with a clinical course distinct from the signs of acute purulent inflammation. Pain syndrome was often of moderate or low intensity, disproportionate to the extent of necrotic foci. Tissue pallor, coldness, and decreased sensitivity were noted as important clinical indicators of microcirculatory disturbances.Local examination revealed necrotic foci covered with gray or black tissues having irregular borders, with minimal inflammatory infiltration in the surrounding tissues. This condition significantly differs from classic purulent processes and exhibits clinical signs characteristic of ischemic necrosis in the context of systemic vasculitis.Many patients presented with persistent ulcers of the oral mucosa, exposed dental alveoli, bone exposure, and sequestra. Unlike odontogenic infections, these symptoms showed poor response to antibiotic therapy.
3. Research Results
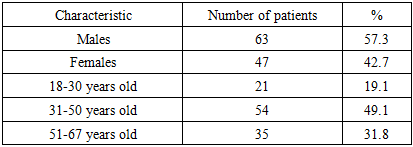
- This study involved a clinical analysis of 110 patients with confirmed systemic vasculitis and purulent-necrotic complications in the maxillofacial region. The patients' ages ranged from 18 to 67 years, with a mean age of 42.8 ± 4.1 years. There were 63 males (57.3%) and 47 females (42.7%). Severe and destructive forms of the disease were observed more frequently in men compared to women.
|
 | Figure 1. Ulcerative-necrotic lesions on the lips and chin |
|
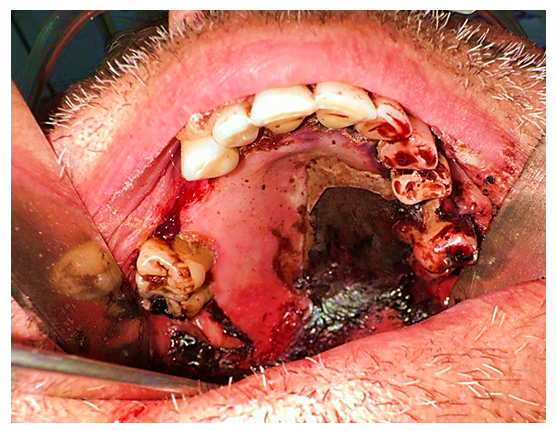 | Figure 2. Necrosis of the maxilla with exposure of the bone structures |
|
|
4. Conclusions
- Endothelial dysfunction, deposition of immune complexes in the vascular wall, activation of the complement system, and necrotic inflammation play a key role in the pathogenesis of these diseases. Clinically, systemic vasculitis manifests with polymorphic signs, which significantly complicates diagnosis in the early stages of the disease. Purulent-necrotic complications developing in the maxillofacial region against the background of systemic vasculitis have a clinically distinct course, and their early detection requires comprehensive clinical diagnostics. The combination of a detailed medical history, thorough clinical examination, differential diagnosis, and instrumental studies is crucial for establishing the correct diagnosis and determining treatment strategies.