-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1563-1566
doi:10.5923/j.ajmms.20261604.03
Received: Feb. 6, 2026; Accepted: Feb. 26, 2026; Published: Apr. 1, 2026

The Role of the Catestatin Biomarker in the Diagnosis of Cardiorenal Syndrome in Patients with Chronic Kidney Disease and Overweight
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDavlatova Nargiza Nugmanovna, Akhmedova Nilufar Sharifovna
Bukhara State Medical Institute, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study is devoted to evaluating the significance of the catestatin biomarker in the early diagnosis of cardiorenal syndrome in patients with overweight and chronic kidney disease. Between 2022 and 2024, comprehensive clinical, laboratory, and instrumental examinations were conducted in 130 patients. Renal function parameters (creatinine, cystatin C, estimated glomerular filtration rate, and albumin-to-creatinine ratio), cardiac stress markers (NT-proBNP, echocardiography), as well as neurohumoral and fibrotic biomarkers (catestatin and galectin-3) were analyzed. The results demonstrated a significant association between elevated catestatin levels, reduced eGFR, and increased NT-proBNP and galectin-3 concentrations. Multivariate analysis confirmed catestatin as an independent predictor of high cardiorenal risk. The use of catestatin expands the possibilities for early detection and risk stratification of cardiorenal syndrome.
Keywords: CKD, Cardiorenal syndrome, Obesity, Catestatin, Biomarker
Cite this paper: Davlatova Nargiza Nugmanovna, Akhmedova Nilufar Sharifovna, The Role of the Catestatin Biomarker in the Diagnosis of Cardiorenal Syndrome in Patients with Chronic Kidney Disease and Overweight, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1563-1566. doi: 10.5923/j.ajmms.20261604.03.
1. Introduction
- Over the past decades, overweight and obesity have become among the most pressing global public health challenges, being recognized as leading risk factors for the development and severe course of cardiovascular and renal diseases. According to the World Health Organization, the prevalence of overweight among the adult population continues to rise annually, contributing to an increased burden of diseases associated with metabolic, hemodynamic, and neurohumoral dysregulation [1,2,3].In the setting of excess body weight, activation of the sympathetic nervous system, hyperactivation of the renin–angiotensin–aldosterone system, increased expression of inflammatory mediators, and endothelial dysfunction intensify the pathogenetic interconnection between cardiac and renal functions. Clinically, this condition manifests as cardiorenal syndrome (CRS), characterized by either progressive renal dysfunction secondary to cardiac impairment or worsening heart failure against the background of renal damage. Numerous studies have explored various biomarkers to achieve early and accurate diagnosis of CRS [4,5,6]. The pathophysiological interactions and feedback mechanisms between the cardiovascular and renal systems are complex and bidirectional, which has attracted increasing scientific interest in recent years [7]. The necessity for a comprehensive review of the epidemiology, pathophysiology, diagnostic tools, and treatment strategies of CRS has been emphasized by the Council on the Kidney in Cardiovascular Disease of the American Heart Association [8,9].Currently, no widely used therapeutic agents based on catestatin are available in routine clinical practice for CRS; however, the development of novel drugs and synthetic analogues is actively ongoing. Further clinical studies evaluating catestatin as both a biomarker and a therapeutic agent are expected to clarify its future clinical prospects [10].Penna et al. (2022) demonstrated that patients with elevated catestatin levels exhibited a 2–3-fold increase in one-year mortality risk, positioning catestatin as a novel prognostic tool in CRS [11]. Experimental studies by Angelone et al. (2021) showed that catestatin administration in murine models of heart failure reduced myocardial inflammation and hypertrophy while improving cardiac function, further supporting its therapeutic potential in CRS [12,13].Thus, catestatin has attracted considerable scientific interest as an important biomarker reflecting the pathophysiology of CRS, with promising diagnostic and prognostic value and potential therapeutic implications. Future studies may address existing gaps and facilitate its broader clinical application [14,15].In Uzbekistan, several studies have investigated the epidemiology of cardiovascular and renal diseases as well as obesity and metabolic syndrome. However, most available research relies on conventional laboratory parameters, while innovative biomarkers reflecting sympathetic neurohumoral regulation, including catestatin, remain insufficiently studied [16,17]. This highlights the lack of national data on the use of catestatin in CRS diagnostics and underscores the scientific novelty and practical relevance of the present study.Aim of the study to propose a clinical and laboratory approach for the early diagnosis, risk stratification, and prediction of disease progression in cardiorenal syndrome among overweight patients using the catestatin biomarker.
2. Materials and Methods
- Study Design and Definition of Cardiorenal Syndrome. This study was designed as a single-center observational prospective cohort study conducted between 2022 and 2024 at the Bukhara филиal of the Republican Specialized Scientific and Practical Center of Cardiology.Cardiorenal syndrome (CRS) was classified according to the American Heart Association and Acute Dialysis Quality Initiative criteria. Based on clinical and laboratory characteristics, patients predominantly corresponded to:• Type 2 CRS – chronic cardiac dysfunction leading to progressive renal impairment• Type 4 CRS – chronic kidney disease contributing to cardiac dysfunctionCRS diagnosis required:• eGFR < 90 mL/min/1.73 m² with evidence of albuminuria• Structural or functional cardiac abnormalities (echocardiographic diastolic dysfunction or elevated NT-proBNP)• Absence of acute kidney injury.A total of 130 patients aged 18–74 years were enrolled (53.8% men, n = 70; 46.2% women, n = 60). The mean age was 52.7 ± 3.5 years. Sample Size Justification. Sample size adequacy was evaluated using power analysis for logistic regression. Based on an anticipated odds ratio of 1.7–2.0 for catestatin and assuming a 30% prevalence of high cardiorenal risk, a minimum of 118 participants was required to achieve 80% statistical power at α = 0.05. Therefore, the inclusion of 130 patients was considered statistically sufficient.Risk Stratification Criteria. Risk groups were defined a priori based on predefined operational criteria:Low Risk• eGFR ≥ 75 mL/min/1.73 m²• NT-proBNP within age-adjusted reference• Catestatin < 3.5 ng/mLModerate Risk• eGFR 45–74 mL/min/1.73 m²• Mild elevation of NT-proBNP• Catestatin 3.5–6.0 ng/mLHigh Risk• eGFR < 45 mL/min/1.73 m²• NT-proBNP > reference• Catestatin > 6.0 ng/mLStratification was predefined before statistical analysis.Catestatin Measurement DetailsSerum catestatin concentration was determined using a commercially available ELISA kit (Cloud-Clone Corp., USA).• Detection range: 0.5–20 ng/mL• Sensitivity: 0.19 ng/mL• Intra-assay coefficient of variation: <8%• Inter-assay coefficient of variation: <10%Galectin-3 was measured using ELISA (R&D Systems, USA) with validated analytical performance.Medication Profile and Confounding FactorsMedication use was recorded and adjusted for in multivariate models:• ACE inhibitors / ARBs – 64%• Beta-blockers – 58%• SGLT2 inhibitors – 29%• Statins – 72%Duration of obesity (mean 9.4 ± 3.2 years) and CKD (mean 4.1 ± 1.8 years) were included as covariates.Inclusion criteria: body mass index ≥ 25 kg/m²; presence of insulin resistance or metabolic syndrome; ischemic heart disease, arterial hypertension, or diastolic dysfunction; eGFR 30–90 ml/min/1.73 m²; presence or borderline values of microalbuminuria/albuminuria (ACR/MAU).Exclusion criteria: acute or severe infections; active malignancy; severe hepatic failure (Child–Pugh C); acute heart failure; acute kidney injury. Clinical assessment included BMI, waist circumference, blood pressure, NYHA functional class, and comorbidities (diabetes mellitus, hypertension, dyslipidemia).Laboratory tests included serum creatinine, cystatin C, eGFR (creatinine- and cystatin C-based), urinary ACR/MAU, NT-proBNP, C-reactive protein, and fibrotic markers (catestatin, galectin-3). Catestatin levels were measured using enzyme-linked immunosorbent assay (ELISA) following manufacturer instructions.All patients underwent echocardiography with assessment of left ventricular ejection fraction, diastolic dysfunction, and chamber dimensions.Statistical analysis was performed using SPSS/Statistica software. Quantitative variables were expressed as mean ± SD. Group comparisons used Student’s t-test or Mann–Whitney U-test. Correlations were assessed by Spearman’s coefficient. Multivariate logistic regression evaluated the independent prognostic value of catestatin, with results expressed as odds ratios and 95% confidence intervals; p < 0.05 was considered statistically significant.
3. Results
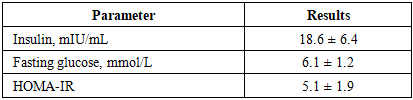
- To assess the metabolic status of the enrolled patients, serum insulin levels and the insulin resistance index (HOMA-IR) were determined. The obtained results demonstrated that insulin resistance was present in the majority of patients, confirming the pronounced manifestation of metabolic disturbances associated with obesity (table 1).
|
|
|

|
4. Conclusions
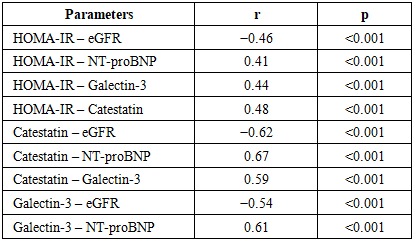
- The results of this study demonstrate that metabolic disturbances, neurohumoral activation, and fibrotic processes are closely interconnected in the pathogenesis of cardiorenal syndrome associated with obesity. As insulin resistance increases, reductions in renal filtration function and elevations in cardiac stress markers develop already at subclinical stages.The negative correlation between catestatin and eGFR, together with its positive associations with NT-proBNP and galectin-3, confirms that enhanced sympathetic neurohumoral activity is directly linked to progression of cardiac and renal dysfunction. Multivariate analysis identified catestatin as an independent predictor of high cardiorenal risk.Thus, the combined assessment of catestatin and galectin-3 represents an effective approach for early diagnosis, risk stratification, and prediction of disease progression in cardiorenal syndrome and provides a strong scientific rationale for their implementation in clinical practice.