-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(4): 1558-1562
doi:10.5923/j.ajmms.20261604.02
Received: Feb. 1, 2026; Accepted: Feb. 26, 2026; Published: Apr. 1, 2026

Features of Pregnancy in Women with Undifferentiated Connective Tissue Dysplasia in the Samarkand Region
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShodikulova Gulandom Zikriyayevna, Yunusova Zarnigor Maksadovna
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

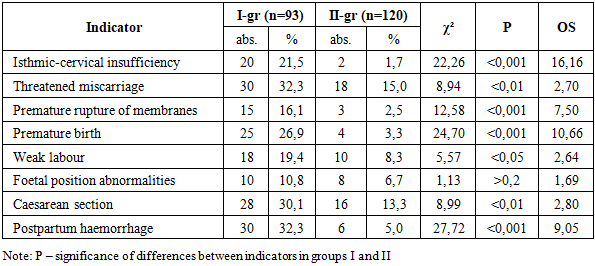
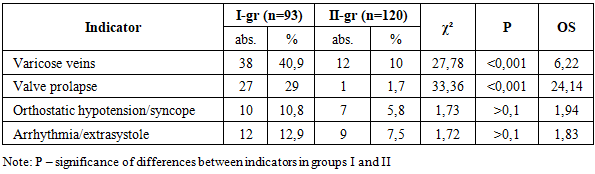
Background. Undifferentiated connective tissue dysplasia (UCTD) is a genetically determined systemic disorder characterized by impaired collagen synthesis and structural organization, affecting the morphofunctional integrity of the uterus, placenta, and vascular wall. In obstetric practice, UCTD is associated with an increased risk of adverse pregnancy outcomes, including miscarriage, premature birth, placental insufficiency, and hemorrhagic complications. Due to the high prevalence of UCTD among women of reproductive age and the absence of unified diagnostic criteria, further investigation of its clinical impact on pregnancy remains relevant. The aim of the present study was to determine the prevalence of UCTD among pregnant women in the Samarkand region and to assess its clinical and obstetric significance. Materials and Methods. A combined retrospective and prospective study was conducted between 2023 and 2025 at Family Polyclinic No. 3 and the Gynecology Department of the Maternity Complex of the Multidisciplinary Clinic of Samarkand State Medical University. Among 3,482 admitted pregnant women, 739 (21.2%) demonstrated clinical signs of UCTD. A prospective cohort of 213 pregnant women was formed, including 93 patients with UCTD and 120 age- and gestation-matched controls. Diagnostic criteria included anamnestic data, Beighton score assessment, clinical phenotypic markers, biochemical indicators of collagen metabolism, and instrumental examinations. Statistical analysis was performed using SPSS software. Differences were evaluated using χ²-test and Student’s t-test, with p < 0.05 considered statistically significant. Results. UCTD was diagnosed in 21.2% of pregnant women. The highest prevalence was observed in women under 25 years (27.5%). Patients with UCTD demonstrated significantly higher rates of obstetric complications, including isthmic-cervical insufficiency (21.5% vs. 1.7%, p < 0.001), threatened miscarriage (32.3% vs. 15.0%, p < 0.01), premature rupture of membranes (16.1% vs. 2.5%, p < 0.001), premature birth (26.9% vs. 3.3%, p < 0.001), and postpartum hemorrhage (32.3% vs. 5.0%, p < 0.001). Somatic manifestations such as varicose veins (40.9% vs. 10%, p < 0.001) and heart valve prolapse (29% vs. 1.7%, p < 0.001) were significantly more frequent in the UCTD group. Conclusion. Pregnancy in women with UCTD is associated with a significantly increased risk of obstetric and somatic complications. The systemic nature of connective tissue insufficiency contributes to impaired cervical competence, vascular fragility, and functional disorders. Early identification and individualized monitoring strategies are essential to reduce adverse perinatal outcomes in this high-risk population.
Keywords: Connective tissue dysplasia, Pregnancy complications, Cervical insufficiency, Premature birth, Joint hypermobility
Cite this paper: Shodikulova Gulandom Zikriyayevna, Yunusova Zarnigor Maksadovna, Features of Pregnancy in Women with Undifferentiated Connective Tissue Dysplasia in the Samarkand Region, American Journal of Medicine and Medical Sciences, Vol. 16 No. 4, 2026, pp. 1558-1562. doi: 10.5923/j.ajmms.20261604.02.
1. Introduction
- Currently, special attention in obstetrics is paid to the problem of managing pregnancy against the background of undifferenciated connective tissue dysplasia (UCTD), which is considered as a systemic disorder affecting the structures that ensure the morphofunctional integrity of the uterus, placenta, and vascular wall [1,2]. Connective tissue diseases are among the significant causes of complicated pregnancies and adverse perinatal outcomes, including premature birth and placental dysfunction. According to the definition by T.I. Kadurina [3], UCTD is a genetically determined disorder of connective tissue development in the embryonic and postnatal periods due to mutations in genes encoding the synthesis and spatial organisation of collagen, elastin and other proteins, leading to homeostasis disorders at the tissue, organ and organism levels [4,5,6,7].The relevance of studying UCTD is due to its high prevalence in the population, which, according to various authors, ranges from 13% to 85.4% [8,9]. Such significant fluctuations in prevalence rates are associated with the lack of uniform diagnostic criteria and different approaches to the identification of phenotypic markers of the disease. The problem is particularly significant because UCTD mainly affects young people, including women of reproductive age [10,11,12]. Therapeutic approaches to the management of pregnant women with UCTD should be based on pathogenetic principles, taking into account the individual characteristics of the patient. Promising areas include the development of personalised medicine and the introduction of new methods of diagnosis and treatment, which served as the theoretical basis for this study.The aim of the study was to determine the incidence of undifferentiated connective tissue dysplasia in pregnant women of the Samarkand region and to study the characteristics of its clinical course.
2. Material and Methods
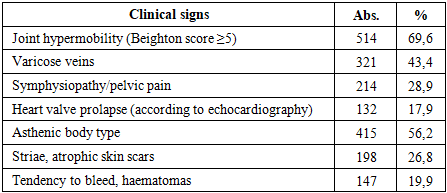
- The study was conducted at Family Polyclinic No. 3 and the Gynaecology Department of the Maternity Complex of the Multidisciplinary Clinic of Samarkand State Medical University between 2023 and 2025. An retrospective analysis of pregnant women admitted to the maternity complex showed that out of 3,482 patients, 739 had signs of UCTD, which is 21.2%. The diagnostic criteria for UCTD included anamnestic data (frequency of spontaneous miscarriages, premature births, family history), clinical signs (asthenic body type, increased joint mobility on the Beighton scale, varicose veins, symphysiopathy, valve prolapse, skin manifestations in the form of striae and atrophic scars). A total of 213 pregnant women were monitored, formed prospective group and divided into two groups depending on the presence of signs of UCTD: group I - 93 patients diagnosed with UCTD; group II - 120 practically healthy pregnant women without clinical and laboratory signs of UCTD, matched by age and gestation period to the main group. Patients in both groups were comparable in terms of key socio-demographic indicators (level of education, social status, marital status). Most of the subjects were in their second trimester of pregnancy (18–24 weeks), which corresponded to the timing of standard screening examinations.The laboratory and instrumental part of the diagnosis included the determination of biochemical markers of collagen metabolism (hydroxyproline, glycosaminoglycans, hyaluronic acid, hyaluronidase activity), as well as indicators of mineral metabolism (Mg²⁺, Ca²⁺, P). A mandatory step was the exclusion of differentiated hereditary collagenopathies, such as Marfan syndrome, Ehlers-Danlos syndrome, imperfect osteogenesis, and others. When analysing the age composition of the examined patients, it was found that the average age of women in group I (with UDCT) was 28.1±0.5 years, in group II – 27.6±0.4 years, with no statistically significant differences between the groups (p>0.05). The age range of patients in the main group was from 18 to 39 years, and in the control group, from 19 to 38 years, which indicates the comparability of the groups in terms of this indicator. The gestational age at the time of inclusion in the study was 18.9±0.6 weeks in group I and 19.4±0.5 weeks in group II, also with no statistically significant differences (p>0.05). Thus, the groups were comparable in terms of age and gestational age.
3. Results of Our Own Research
- When assessing obstetric history, it was found that the average number of pregnancies in patients with UCTD was 1.8±0.1, which was comparable to the control group – 1.7±0.1 (p>0.05). The number of births in group I was significantly lower (1.0±0.1) than in group II (1.3±0.1; p<0.05), reflecting the reproductive function characteristics of women with signs of connective tissue dysplasia.Particular attention was drawn to the rate of spontaneous miscarriages: in group I, it was 0.82±0.1, which was more than twice as high as the corresponding rate in the control group – 0.43±0.05 (p<0.001). This fact indicates the significant role of UCTD in the formation of adverse outcomes in the early stages of pregnancy. The body mass index before pregnancy in both groups did not differ significantly and was 21.4±0.3 kg/m² in the main group and 22.0±0.3 kg/m² in the control group (p>0.05). Thus, the compared groups were homogeneous in terms of age, gestational age, body mass index, and socio-demographic characteristics. Differences were identified in obstetric history indicators. Patients with UCTD had significantly fewer births and more spontaneous miscarriages, indicating significant reproductive risks in this category of women.An analysis of the medical records of pregnant women admitted to the maternity complex in 2024 showed (Table 1) that out of 3,482 patients, signs of UCTD were detected in 739 women, which accounted for 21.2%. Thus, one in five pregnant women admitted had clinical or laboratory-instrumental signs of CD. The obtained CD frequency rate is consistent with the literature data, according to which the prevalence of this pathology in women of reproductive age ranges from 20 to 30%. This confirms the high significance of connective tissue dysplasia as a background condition that can affect the course of pregnancy and its outcomes.
|

|
|
|
4. Conclusions
- Thus, the analysis showed that pregnancy in women with undifferentiated connective tissue dysplasia occurs against a background of a significantly higher frequency of obstetric complications. The most frequently recorded complications were isthmic-cervical insufficiency, threatened miscarriage, premature birth, premature rupture of the membranes, and postpartum haemorrhage. These complications have a direct pathogenetic link to connective tissue insufficiency. Somatic manifestations in patients with UCTD were characterised by a high frequency of varicose veins and heart valve prolapse, confirming the systemic nature of dysplastic disorders. In addition, functional disorders were noted, the most pronounced of which were symphysiopathy and dermatological manifestations (stretch marks and atrophic skin scars). The combination of the data obtained indicates that the clinical manifestations of UCTD in pregnant women have a pronounced obstetric and perinatal significance, determining a high risk of adverse pregnancy outcomes and the need for a differentiated approach to monitoring, prevention, and correction of complications in this category of patients.