-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1298-1306
doi:10.5923/j.ajmms.20261603.93
Received: Feb. 20, 2026; Accepted: Mar. 12, 2026; Published: Mar. 23, 2026

Clinico-Immunological Predictors of Early Graft Dysfunction and Their Relevance for Rehabilitation of Liver and Kidney Transplant Recipients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdurakhmanov Mumin Marimovich
National Medical Center, Uzbekistan
Correspondence to: Abdurakhmanov Mumin Marimovich, National Medical Center, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Liver and kidney transplantation are standard treatments for end-stage organ disease; however, early graft dysfunction (EGD) and delayed graft function (DGF) remain important clinical problems associated with ischemia-reperfusion injury, immune activation, and patient-related factors. Objective. To summarize clinico-immunological predictors of early graft dysfunction and evaluate their role in optimizing rehabilitation strategies. Materials and Methods. A narrative review was conducted based on current literature, including guidelines, clinical studies, and systematic reviews related to transplantation, immunology, biomarkers, and rehabilitation. Results. Early graft dysfunction represents a multifactorial condition driven by ischemia-reperfusion injury, inflammatory responses, and immune mechanisms. Biomarkers such as IL-6, TNF-α, CRP, and NGAL contribute to early risk assessment. Functional factors, including frailty and sarcopenia, significantly influence postoperative recovery. Rehabilitation approaches improve outcomes but remain insufficiently individualized. Conclusions. Clinico-immunological predictors can support personalized rehabilitation strategies after transplantation. An integrated approach combining biological and functional parameters is essential for improving patient outcomes.
Keywords: Liver transplantation, Kidney transplantation, Early graft dysfunction, Delayed graft function, Ischemia-reperfusion injury, Inflammation, Biomarkers, Frailty, Sarcopenia, Rehabilitation, Prehabilitation
Cite this paper: Abdurakhmanov Mumin Marimovich, Clinico-Immunological Predictors of Early Graft Dysfunction and Their Relevance for Rehabilitation of Liver and Kidney Transplant Recipients, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1298-1306. doi: 10.5923/j.ajmms.20261603.93.
1. Introduction
- Liver and kidney transplantation are among the most successful achievements of modern clinical medicine because they offer a durable survival benefit in patients with otherwise irreversible end-stage organ disease [1-6]. Contemporary registry data show that one-year patient and graft survival have improved substantially due to advances in donor selection, organ preservation, anesthetic management, critical care, immunosuppressive therapy, and post-transplant surveillance [1,2,7,8]. These gains, however, have shifted the focus of transplantation medicine. Once short-term survival becomes more predictable, the major determinants of outcome move toward the quality of the early postoperative course, the resilience of the graft-recipient system under inflammatory stress, and the speed and completeness of functional recovery.The early post-transplant period is biologically dense. It is the phase in which the organ experiences reperfusion after a period of procurement, cold storage, and implantation; in which the recipient encounters a major surgical insult, profound metabolic changes, fluctuating hemodynamics, and exposure to high-dose immunosuppression; and in which the first signals of both graft adaptation and graft injury become clinically visible [9-16]. In liver transplantation, early allograft dysfunction has emerged as a robust surrogate of suboptimal graft recovery, with well-recognized associations with intensive care burden, renal impairment, and inferior graft survival [9-11,15]. In kidney transplantation, delayed graft function remains a central challenge because it is associated not only with prolonged hospitalization and higher resource use but also with an increased risk of acute rejection and poorer long-term graft survival [12-16].From a mechanistic standpoint, early graft dysfunction is not reducible to a single laboratory threshold. It is the clinical expression of several converging pathological processes, among which ischemia-reperfusion injury is foundational [17-27]. Ischemia depletes cellular energy stores, disrupts ion homeostasis, and primes endothelial and parenchymal cells for injury. Reperfusion then restores oxygen delivery in a manner that paradoxically intensifies cellular damage through oxidative stress, mitochondrial dysfunction, endothelial activation, leukocyte recruitment, and microcirculatory collapse [18-23]. Organ preservation strategies and machine perfusion technologies can attenuate this injury, but they do not abolish it [24-27]. Consequently, the early behavior of the graft depends on how successfully the organ and host contain the reperfusion-induced inflammatory storm.This storm is both inflammatory and immunological. Damage-associated molecular patterns released from injured cells activate innate immune pathways and initiate a cytokine-dominated response in which IL-6, TNF-alpha, IL-1 family mediators, and chemokine networks play central roles [28-35]. In the transplant setting, this sterile inflammatory response is particularly important because it overlaps with alloimmune recognition. The same tissue injury that recruits innate immune cells also enhances antigen presentation, lowers activation thresholds for adaptive immunity, and contributes to the development of donor-specific immune responses [36-49]. Accordingly, early graft dysfunction and immunological risk should not be analyzed in isolation. They are interconnected elements of one clinical continuum that influences both graft performance and patient recovery.At the same time, modern transplantation medicine can no longer define success solely as laboratory normalization or absence of rejection. A large body of work now demonstrates that transplant recipients frequently enter surgery with substantial frailty, sarcopenia, reduced exercise tolerance, and psychosocial vulnerability, and that these impairments often persist after technically successful transplantation [59-67]. In both liver and kidney transplantation, functional reserve strongly shapes the capacity to withstand the postoperative inflammatory burden, resume mobility, participate in rehabilitation, and regain quality of life [59-67]. This means that biological graft recovery and whole-patient recovery are related but not identical processes.For this reason, rehabilitation has become an increasingly important component of transplant care [68-85]. Early mobilization, structured exercise, respiratory training, nutritional support, and multimodal rehabilitation can improve exercise capacity, functional independence, and patient-reported outcomes [68-85]. Yet most rehabilitation pathways still rely on broad clinical judgment rather than on a formal integration of graft biology, inflammatory risk, and functional reserve. The present review addresses this gap by synthesizing current evidence on clinico-immunological predictors of early graft dysfunction after liver and kidney transplantation and by examining how these predictors can inform personalized rehabilitation strategies.
2. Materials and Methods
- Review designThis article was designed as a narrative review presented in an IMRAD format. The rationale for this choice was twofold. First, the target topic spans mechanistic immunology, transplant surgery, perioperative medicine, functional medicine, and rehabilitation science; therefore, an interpretive synthesis is more suitable than a narrowly protocolized systematic review. Second, structuring the manuscript according to IMRAD allows the review to conform to the expectations of many international journals while maintaining transparency regarding how evidence was selected, grouped, and interpreted.Evidence sources and eligibility approachThe review was based on the source collection supplied by the authors. That collection included registry reports, guidelines, consensus statements, foundational textbooks, clinical reviews, mechanistic experimental studies, prospective observational cohorts, biopsy and molecular monitoring studies, randomized exercise trials, and systematic reviews relevant to liver and kidney transplantation. Priority was given to sources that addressed at least one of four core domains: (1) definitions and clinical impact of early graft dysfunction or delayed graft function; (2) biological predictors, especially ischemia-reperfusion injury, inflammatory mediators, alloimmunity, and biomarkers; (3) functional predictors, including frailty, sarcopenia, and exercise intolerance; and (4) rehabilitation, prehabilitation, and continuum-of-care models. English-language publications from 1990 to 2024 were emphasized, with older landmark sources retained when they were conceptually indispensable.Analytical frameworkThe retrieved evidence was analyzed using a translational framework rather than a disease-only framework. Instead of treating liver and kidney transplantation as entirely separate narratives, the evidence was organized around shared biological and clinical axes: graft injury, inflammatory activation, immune risk, monitoring tools, functional reserve, and response to rehabilitation. Within each axis, similarities and organ-specific distinctions were identified. This approach made it possible to examine whether the same predictor that forecasts early graft dysfunction may also have implications for rehabilitation timing, intensity, safety, or monitoring burden.Data synthesis strategyThe synthesis proceeded in three stages. First, the literature was grouped into thematic clusters: state of transplantation, early graft dysfunction definitions, ischemia-reperfusion injury, innate and adaptive immune responses, immunogenetics, biomarkers, functional impairment, rehabilitation, and prehabilitation. Second, the clinical meaning of each cluster was interpreted with specific attention to early recovery after transplantation. Third, the evidence was integrated into a practical model that links clinico-immunological risk factors with rehabilitation decision-making. Because this was a narrative review, no quantitative meta-analysis was attempted and no pooled effect sizes were calculated.
3. Results
- Contemporary state of liver and kidney transplantation and why the early phase mattersThe current state of liver and kidney transplantation is characterized by a paradox. On the one hand, transplantation outcomes are better than at any previous time, and registry data confirm the durability of the procedure as a life-saving intervention in both organ systems [1-8]. Kidney transplantation remains the most frequent solid-organ transplant worldwide and offers major survival and cardiovascular advantages over long-term dialysis, while liver transplantation remains the definitive treatment for end-stage liver failure, selected malignancies, and specific metabolic disorders [1-8]. On the other hand, these improved outcomes have raised expectations. In the modern era, clinicians, patients, and health systems expect not only survival but also stable graft function, short intensive-care stays, fast mobilization, lower complication rates, and restoration of meaningful daily function.This shift in expectations has made the early post-transplant period the critical transition zone between operative success and durable recovery [7-16]. The early course shapes not only whether the graft survives but also how the recipient experiences the first weeks after surgery: whether renal replacement therapy is needed, whether ventilation is prolonged, whether infections occur, whether mobility can be resumed, and whether the patient is strong enough to participate in active recovery. For this reason, the biological events of the early phase must be understood as recovery-limiting or recovery-facilitating forces, rather than as transplant-specific laboratory phenomena only.Early graft dysfunction as a clinically meaningful syndromeThe term early graft dysfunction captures the inability of a transplanted organ to achieve stable functional recovery soon after implantation. In liver transplantation, the most widely accepted clinical definition is the one proposed by Olthoff and colleagues, which uses bilirubin, international normalized ratio, and marked aminotransferase elevation during the first postoperative week [9]. This definition gained traction because it is simple, reproducible, and clinically relevant. Subsequent studies showed that patients with early allograft dysfunction have longer intensive-care and hospital stays, greater risk of renal impairment, and worse short- and long-term outcomes [10,11,15]. Importantly, the syndrome is not identical to primary nonfunction; rather, it represents a spectrum of impaired adaptation, ranging from transient biochemical disturbance to more consequential organ instability.In kidney transplantation, delayed graft function has traditionally been defined as the need for dialysis in the first postoperative week [12]. Although this definition is easy to apply, it has well-known limitations because dialysis decisions are influenced by local practice patterns, fluid management strategies, and recipient comorbidity. Systematic reviews have demonstrated marked heterogeneity in DGF definitions, with many studies proposing alternative criteria such as creatinine reduction ratios or urine output-based thresholds [13,16]. Despite this definitional variability, the clinical message is consistent: delayed graft function marks a graft-recipient dyad under stress and predicts more complex postoperative care, higher rejection risk, and inferior long-term graft survival [12-16].The prognostic importance of early graft dysfunction rests on the fact that it integrates several risk layers into a single observable phenotype. It is affected by donor quality, procurement conditions, ischemia time, reperfusion injury, recipient inflammation, hemodynamic instability, and immunological activation [9-16]. Because it summarizes these multiple dimensions, it is clinically more informative than any one isolated variable. At the same time, its usefulness is limited if it is treated as the final diagnosis rather than as a signpost toward deeper biological and rehabilitative assessment.Ischemia-reperfusion injury as the substrate of early graft dysfunctionThe most consistent biological substrate of early graft dysfunction is ischemia-reperfusion injury [17-27]. During procurement and preservation, the graft is subjected to hypoxia, ATP depletion, acidosis, ionic disequilibrium, membrane instability, and mitochondrial stress [17-23]. In the liver, hepatocytes, cholangiocytes, sinusoidal endothelial cells, and Kupffer cells all respond differently to ischemia, creating a heterogeneous pattern of injury. In the kidney, tubular epithelial cells, endothelial cells, and the microvascular network are central targets, particularly within the corticomedullary region, where oxygen tension is already physiologically vulnerable [21-23]. By the time reperfusion occurs, the graft is therefore not a neutral organ awaiting recovery but a metabolically fragile tissue primed for inflammatory amplification.Reperfusion restores oxygen supply, but this restoration paradoxically accelerates injury. Reactive oxygen species formation increases, mitochondrial permeability is disturbed, endothelial cells upregulate adhesion molecules, and complement and coagulation pathways become activated [18-23]. In practical terms, this means that the graft may receive blood flow macroscopically while remaining functionally hypoperfused at the microcirculatory level. The phenomenon of no-reflow, recognized particularly in hepatic ischemia-reperfusion injury, exemplifies how vascular patency does not automatically translate into tissue-level recovery [19,20]. Similar principles apply to kidney transplantation, where endothelial swelling, leukocyte plugging, and interstitial edema can perpetuate tubular injury even after anastomotic success.Donor and preservation variables strongly modify this process. Expanded-criteria donors, steatotic livers, prolonged cold ischemia, donor age, and suboptimal preservation intensify the likelihood that reperfusion will produce clinically meaningful dysfunction [24-27]. This is the rationale behind the rapid expansion of machine perfusion technologies. Normothermic, hypothermic oxygenated, and other dynamic preservation strategies do more than preserve the organ; they partly recondition metabolism, improve energy status, and reduce downstream inflammatory injury [24-27]. Yet even with these technologies, the recipient’s postoperative trajectory remains partly determined by the degree of tissue injury already embedded in the graft.Immunogenetic factors and why biological heterogeneity matters clinicallyImmunogenetic compatibility modifies both the likelihood and the expression of post-transplant immune injury [41-49]. In kidney transplantation, the association between HLA mismatch burden and inferior graft survival is robust and longstanding [46,47]. More mismatches usually mean more alloimmune opportunities, greater immunological vigilance, and potentially more intensive monitoring. In liver transplantation, the signal is more nuanced, but donor-specific HLA antibodies, particularly when persistent or de novo, are increasingly linked to endothelial injury and adverse outcomes [43,48,49].Beyond classical HLA matching, polymorphisms affecting cytokine pathways, innate immune receptors, adhesion molecules, and repair responses may help explain why clinically similar patients experience markedly different inflammatory phenotypes after transplantation. Although these polymorphisms are not yet used routinely in rehabilitation planning, they remind clinicians that early recovery trajectories are biologically heterogeneous. Two recipients with apparently similar operations may differ substantially in inflammatory amplification, catabolic burden, and susceptibility to complications. This biological heterogeneity strengthens the argument against a one-size-fits-all rehabilitation model.Biomarkers of early graft injury and systemic inflammationThe reviewed literature supports a layered biomarker approach rather than reliance on any single marker [50-58]. At the simplest level, standard biochemical tests remain indispensable. Bilirubin, aminotransferases, INR, creatinine, urine output, and dialysis requirement continue to define clinically significant dysfunction because they reflect organ performance directly [9,12-16]. However, these variables often change only after clinically relevant injury is already underway. For this reason, attention has turned toward mechanistically informative biomarkers that can signal tissue injury and inflammatory risk earlier.In kidney transplantation, urinary and plasma NGAL, IL-18, and other tubular injury markers help identify patients at risk of delayed graft function before conventional criteria are fully met [50,51]. In both organ systems, inflammatory indices such as high-sensitivity C-reactive protein and neutrophil-to-lymphocyte ratio provide inexpensive and repeatable indicators of systemic inflammatory load. They are nonspecific, but their clinical value lies in trend recognition, integration with graft parameters, and ease of implementation in routine practice. Cytokines such as IL-6 and TNF-alpha offer closer proximity to mechanism, although their widespread adoption is limited by assay availability and standardization [35].Donor-derived cell-free DNA is one of the most promising translational tools because it quantifies graft-derived injury in a noninvasive manner [52-55]. Studies in kidney and liver transplantation suggest that dd-cfDNA can detect graft damage and rejection earlier than some traditional approaches, although interpretation still requires careful clinical context [52-55]. Molecular diagnostics based on gene-expression signatures or transcriptomic biopsy analyses further expand the diagnostic horizon, particularly in kidney transplantation, where they help separate immune-mediated injury from other causes of dysfunction [56-58]. Yet the rehabilitation relevance of these tools remains underdeveloped. They are commonly viewed as surveillance instruments rather than as guides for individualized recovery planning.Translational synthesis: linking clinico-immunological predictors with rehabilitation decisionsThe central finding of this review is that clinico-immunological predictors of early graft dysfunction have immediate relevance for rehabilitation planning. Inflammation-heavy postoperative phenotypes—characterized by high IL-6 or TNF-alpha levels, elevated inflammatory indices, delayed graft recovery, fluid instability, and heightened immunological concern—are not merely “sicker versions” of otherwise similar patients. They are biologically distinct patients whose rehabilitation tolerance is different. They may need slower progression of upright activity, tighter hemodynamic and oxygenation monitoring during exercise, more aggressive nutritional intervention, careful fluid balance management, and closer coordination between transplant physicians, intensivists, nutrition specialists, and rehabilitation staff.
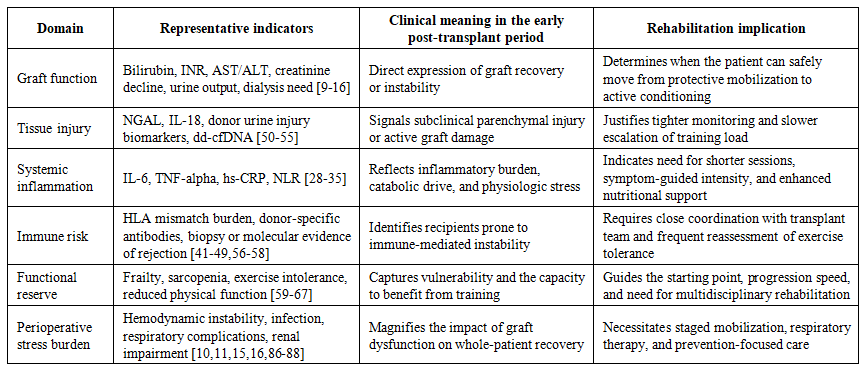 | Table 1. Major clinico-immunological predictors of early graft dysfunction and their rehabilitation implications |
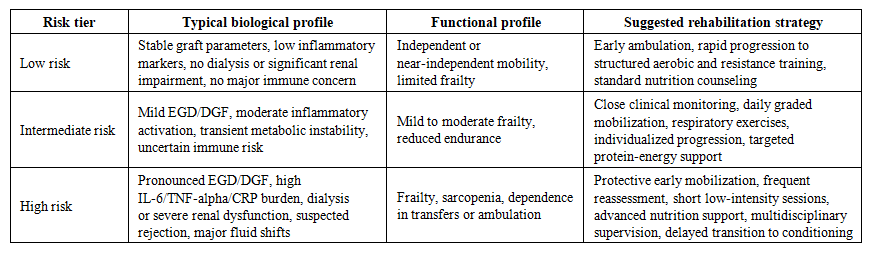 | Table 2. Conceptual risk-adapted rehabilitation model for liver and kidney transplant recipients |
4. Discussion
- This review brings together two literatures that are often discussed separately: the biological literature on early graft dysfunction and the rehabilitation literature on functional recovery after transplantation. The first literature is rich in pathophysiology, biomarkers, and monitoring techniques; the second is rich in exercise studies, prehabilitation concepts, and patient-centered outcomes [9-58,68-85]. What has been insufficiently articulated is that these are not parallel stories. The same inflammatory and immune processes that determine whether a graft recovers promptly also determine whether the patient can sit, stand, breathe deeply, train safely, preserve muscle mass, and regain autonomy. Accordingly, graft biology is rehabilitation biology.From a clinical standpoint, one of the strongest messages of the available evidence is that early graft dysfunction should be operationalized as a rehabilitation-relevant syndrome. When a liver recipient meets criteria for early allograft dysfunction or a kidney recipient develops delayed graft function, the consequences extend beyond transplant monitoring. These patients are more likely to experience catabolism, fluid shifts, prolonged intensive-care exposure, infectious complications, renal or pulmonary cross-talk, treatment escalation, and psychological stress [10-16,86-88]. Each of these factors alters rehabilitation timing, intensity, and achievable goals. A biologically informed rehabilitation model would therefore treat early graft dysfunction as an automatic signal for intensified multidisciplinary assessment rather than as a problem confined to the transplant team.A second key point is that simple, widely available markers may have more rehabilitation value than they are currently given credit for. High-sensitivity CRP, neutrophil-to-lymphocyte ratio, creatinine trajectory, dialysis requirement, bilirubin, INR, and aminotransferase peaks are accessible in most transplant centers. Although they lack the mechanistic precision of dd-cfDNA or transcriptomics, they can still guide recovery planning when interpreted serially and in context. A recipient with persistent inflammatory elevation, poor creatinine decline, and marked frailty should not automatically follow the same mobilization pathway as a recipient with rapidly improving laboratory results and preserved functional reserve. Therefore, even before advanced biomarker platforms become universal, a pragmatic risk-adapted rehabilitation approach is already feasible.The third major implication concerns prehabilitation and longitudinal care. The reviewed evidence supports the concept that early postoperative recovery is partly determined before the operation through baseline frailty, sarcopenia, nutrition, and psychological preparedness [61-67,77-81]. This argues against viewing postoperative rehabilitation as a rescue intervention applied only after complications have occurred. Instead, transplant programs should conceptualize recovery as a continuum beginning on the waitlist. Functional assessment, nutritional screening, and exercise counseling before transplantation can be paired with postoperative biologic monitoring to produce a more coherent care pathway. Such a pathway is especially relevant in liver and kidney transplantation, where preoperative deconditioning is common and can be profound.Despite these insights, the evidence base has important limitations. Rehabilitation studies often enroll small numbers of recipients, begin after the most unstable postoperative period, or use heterogeneous outcomes that make direct comparison difficult [73-76,80,81,84,85]. Biomarker studies, by contrast, often focus on diagnostic discrimination rather than on how marker trajectories should influence bedside rehabilitation decisions [50-58]. Mechanistic studies clarify biological plausibility but do not by themselves define exercise prescriptions or multidisciplinary recovery algorithms [28-49]. The field therefore needs prospective studies in which biological risk markers and rehabilitation endpoints are measured together. Such studies should test whether a biomarker-informed rehabilitation pathway improves length of stay, complication rates, muscle preservation, functional independence, readmissions, and quality of life.A further area of interest is the adaptation of these concepts to different healthcare settings. Much of the current evidence derives from high-volume transplant centers with access to specialized monitoring, standardized perioperative pathways, and dedicated rehabilitation resources. In many national contexts, including emerging transplant systems, sophisticated molecular tests may be unavailable or too costly for routine use. This does not negate the value of personalized rehabilitation; rather, it highlights the need for scalable models built on a tiered set of predictors. A core package may include conventional graft-function tests, inflammatory indices, frailty screening, and nutritional assessment, while more advanced centers add cytokine panels, donor-specific antibody monitoring, or cell-free DNA assays. The principle of stratified recovery can therefore be preserved even when technology varies.Finally, the translational opportunity lies in moving from descriptive associations to actionable pathways. The literature already tells us that ischemia-reperfusion injury initiates a danger-signal-driven inflammatory cascade, that immune dysregulation worsens graft instability, that frailty and sarcopenia lower resilience, and that rehabilitation can improve function [17-85]. The next step is to connect these facts into operational care. A transplant center should be able to say, for example, that recipients with a defined inflammatory and functional profile will receive a particular intensity of mobilization, a specific nutrition target, and a predefined reassessment schedule. Only then will clinico-immunological predictors become true tools of rehabilitation medicine rather than merely interesting correlates of graft outcome.
5. Conclusions
- Early graft dysfunction after liver and kidney transplantation is a multidimensional syndrome in which ischemia-reperfusion injury, innate inflammatory activation, alloimmune mechanisms, donor and preservation variables, and recipient vulnerability converge. The evidence reviewed here indicates that these clinico-immunological processes are highly relevant to rehabilitation because they shape catabolic burden, hemodynamic stability, respiratory function, muscular recovery, and the capacity to tolerate progressive activity.The most useful conceptual shift is to view post-transplant rehabilitation as a biologically informed continuum rather than a standard postoperative routine. In practice, this means integrating graft-function measures, inflammatory biomarkers, immune-risk indicators, frailty, sarcopenia, and nutrition into a single recovery algorithm. Such an approach would allow early and safer mobilization for low-risk recipients while protecting high-risk recipients from under-monitoring and poorly timed exercise escalation.Future research should prospectively validate stratified rehabilitation models that combine clinico-immunological predictors with meaningful recovery endpoints. Until such evidence is available, transplant programs can already improve care by adopting a pragmatic, multidisciplinary, risk-adapted framework in which the biology of the graft and the biology of functional recovery are assessed together.