-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1294-1297
doi:10.5923/j.ajmms.20261603.92
Received: Feb. 27, 2026; Accepted: Mar. 16, 2026; Published: Mar. 23, 2026

Seasonal Forensic Medical Aspects of Myocardial Histological Changes in Individuals Who Died of Ischemic Heart Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNarzikulov Uchkun Ziyadullayevich, Djurayev Ilkhom Gulyamovich, Sabirov Djakhongir Ruziyevich
National Medical Center, Samarkand State Medical University Uzbekistan, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article analyzes the forensic aspects of histological changes observed in the myocardium of individuals who died from ischemic heart disease (IHD) during the winter season. Cases with a preliminary diagnosis of IHD were examined during the forensic medical examination process. According to the histological analysis results, dystrophic and necrobiotic changes in cardiomyocytes, increased cytoplasmic eosinophilia, nuclear hyperchromia and polymorphism, interstitial edema, and perivascular congestion predominated in the winter. Additionally, muscle fiber disorganization and increased connective tissue were assessed as signs of remodeling in the context of a chronic ischemic process.
Keywords: Ischemic heart disease, Winter season, Myocardium, Histological changes, Ischemic-dystrophic process, Interstitial edema, Perivascular congestion, Forensic medical examination, Sudden death
Cite this paper: Narzikulov Uchkun Ziyadullayevich, Djurayev Ilkhom Gulyamovich, Sabirov Djakhongir Ruziyevich, Seasonal Forensic Medical Aspects of Myocardial Histological Changes in Individuals Who Died of Ischemic Heart Disease, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1294-1297. doi: 10.5923/j.ajmms.20261603.92.
1. Introduction
- Global climate change is not only raising average air temperatures but also increasing the frequency and intensity of extreme weather events-such as heavy precipitation, thunderstorms, and cyclones. These processes negatively affect human health in several ways and are causing increases in morbidity and mortality [9].Furthermore, it is projected that the number of heat-related deaths will increase further with future rises in climate temperatures. The 2024 edition of the Lancet Countdown report noted an excessively high number of heat-related deaths among people aged 65 and older in 2023, further highlighting the importance of adaptation measures [9]. It is now recognized that climate change is causing over 150,000 premature deaths globally each year, through direct effects and the exacerbation of environmental problems [5,6,7,8].A hygienic assessment of the impact of weather conditions on public health not only allows for an understanding of the objective laws of nature but also makes it possible to identify the mechanisms by which environmental factors affect the human body and public health. Through these approaches, it will be possible to develop standards and sanitary and hygienic measures aimed at optimizing living conditions, quality of life, and human activity [2,6].Furthermore, the implementation of hygienic monitoring and forecasting systems to minimize the negative impacts of weather and environmental conditions is of great importance. For example, sudden temperature changes, increased humidity, or high concentrations of harmful substances in the air can all lead to an increase in cardiovascular, respiratory, and allergic diseases among the population [3,7]. In this regard, modern sanitary and hygienic measures must be aimed not only at preventing the spread of infections but also at preventing diseases related to atmospheric conditions [1].Thus, international research conducted in recent years has highlighted the need for modern morphological techniques, such as confocal microscopy, that expand forensic diagnostic capabilities in sudden death cases and increase the accuracy and reliability of expert conclusions.Study objective: To determine the macroscopic and microscopic morphological changes in the myocardium of individuals who died from ischemic heart disease during the winter season, to assess their distinctive characteristics and to scientifically substantiate, from a forensic medicine perspective, the ischemic-hypertrophic and interstitial processes characteristic of the winter season.
2. Materials and Methods
- Materials from forensic medical autopsies performed on cases of sudden death associated with ischemic heart disease were obtained. A total of 196 cases of sudden death from various seasons were included in the study. All cases were studied at the Samarkand branch of the Republican Scientific and Practical Center for Forensic Medicine from 2021 to 2025.The material obtained for examination was fixed in a 10% neutral formalin solution and stored at a temperature of +7°C to +20°C in conditions protected from the adverse effects of air, moisture, and light. Subsequently, the samples were dehydrated in a water bath at 37°C, passed through alcohol and toluene, embedded in paraffin, and stained using standard methods. Microslides were examined using a NanoZoomer scanner microscope (REF C13140-21, S/N 000198, Hamamatsu Photonics, Japan). Histomorphometric analyses were performed using the NDP. View 2.0 and Qu00.0url software packages on a scanner with a 7× ocular and objectives ranging from 8× to 40×. Micrographs of the histological specimens were also obtained with this scanner using NDP. Microphotographs of the histological preparations were obtained using NDP. View 2.0 and Qu00.0url software. Statistical analysis of the results was performed on a Pentium-IV computer using Microsoft Office Excel 2021, and Student's t-test was applied.
3. Research Results
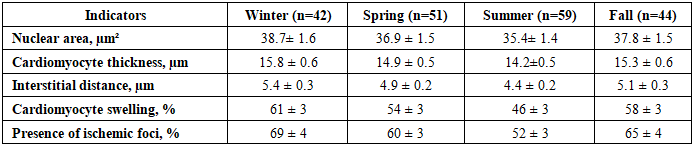
- In this study, through morphometric analysis of histological sections of the left and right ventricles of the heart, the parameters of the nuclei, the thickness of the cardiomyocytes, and the distance between muscle fibers were determined. Based on the obtained data, the relationships between nuclear area and cardiomyocyte thickness and interstitial distance were calculated. In the left ventricle, significant differences were identified in the cardiomyocyte nuclear domain in cases of IHD (Table 1).
|
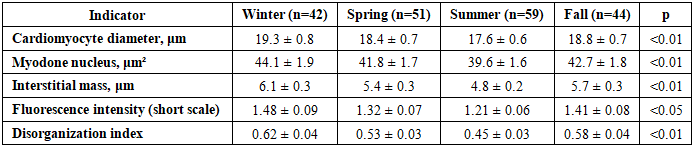
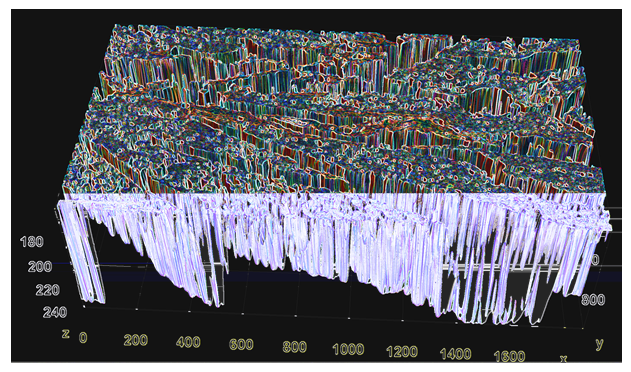 | Figure 1. Confocal multiplex morphometric imaging of the left ventricular myocardium, showing the volumetric measurements of muscle bundles and interstitial stroma. Stain: Shiff. Size: 10 × 10 |
|
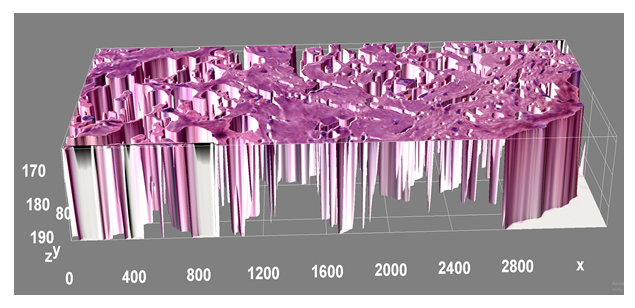 | Figure 2. Confocal multiplex morphometric imaging of the tangential section of the anterior lateral wall of the right ventricle showing the volumetric measurements of muscle bundles and interstitial stroma. Stain: G.E. Scale: 10×10 |
4. Conclusions
- The macroscopic and morphometric indicators of the heart in cases of sudden death associated with ischemic heart disease were found to be variable according to the seasons. In winter, the mean heart weight was 420 g, while in summer it was 380 g (p < 0.05). Additionally, the left ventricular wall thickness was 1.6 cm in winter and 1.4 cm in summer, indicating that hypertrophic remodeling processes are more pronounced in winter.Micromorphometric analysis of the left and right ventricular myocardium revealed a clear seasonal pattern. In winter, the nuclear area was 44.1 µm², compared to 39.6 µm² in summer (p < 0.01), and ischemic foci were observed in 74% and 55% of cases, respectively. This confirms that the ischemic-dystrophic changes were more pronounced in winter.