-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1289-1293
doi:10.5923/j.ajmms.20261603.91
Received: Feb. 12, 2026; Accepted: Mar. 8, 2026; Published: Mar. 23, 2026

Early Prediction and Severity Assessment of Cardiovascular Complications in Comorbid Coronary Heart Disease Based on Acid-Base Balance and Hemostasis Biomarkers
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudova L. I., Naimov F. F.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Makhmudova L. I., Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In the study, the indicators of the acid-base balance and hemostasis system in comorbid conditions with coronary heart disease were studied. With an increase in the level of comorbidity, a tendency towards metabolic acidosis and an increase in hypercoagulation changes were revealed. The highest imbalance was noted in the group of CHD+AH+DM2+obesity (p<0.001). In patients with complications, low pH and HCO3−, high levels of fibrinogen and D-dimer were noted (p<0.01). The obtained results indicate the expediency of using biomarkers of ABB and hemostasis in early prediction and risk stratification. The obtained results indicate the expediency of using biomarkers of blood pressure and hemostasis in the stratification of clinical risk and early prediction of complications.
Keywords: Ischemic heart disease, Comorbid conditions, Arterial hypertension, Type 2 diabetes mellitus, Obesity, Acid-base balance, Metabolic acidosis, Hemostasis system
Cite this paper: Makhmudova L. I., Naimov F. F., Early Prediction and Severity Assessment of Cardiovascular Complications in Comorbid Coronary Heart Disease Based on Acid-Base Balance and Hemostasis Biomarkers, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1289-1293. doi: 10.5923/j.ajmms.20261603.91.
Article Outline
1. Introduction
- Coronary heart disease (CHD) remains one of the leading causes of mortality and disability worldwide [1]. In the development of CHD, myocardial ischemia, endothelial dysfunction, inflammation, and thrombogenesis manifest themselves as interconnected pathogenetic mechanisms [2]. Especially in the presence of comorbid conditions (arterial hypertension, diabetes mellitus, obesity), metabolic disorders deepen, and changes in the acid-base balance (ABB) and hemostasis system are observed [3].It has been noted in the literature that metabolic acidosis or subclinical ABB imbalance can exacerbate hypercoagulation, increase platelet activity, and affect the fibrinolysis system [4]. At the same time, biomarkers of hemostasis - D-dimer, fibrinogen, APTT and other indicators - have important prognostic significance in assessing the severity of CHD and the risk of complications [5].Therefore, the study of the relationship between ABB indicators and biomarkers of the hemostasis system in comorbid conditions with CHD, the assessment of their clinical significance, and their use in risk stratification is a pressing issue.The purpose of the study was to determine the relationship between acid-base indicators (pH, pCO2, HCO3, BE) and blood hemostasis biomarkers (D-dimer, fibrinogen, APTT, PTI, platelets) in comorbid conditions with coronary heart disease, as well as to scientifically substantiate their significance in assessing the severity and clinical course of the disease.
2. Material and Methods
- The study was conducted on 120 patients with coronary heart disease (CHD) who were treated in the cardiology department of the Bukhara Regional Multidisciplinary Medical Center. Patients were divided into 3 groups according to comorbid conditions: 1st group - CHD + arterial hypertension (AH); 2nd group - CHD + type 2 diabetes mellitus (DM2) + obesity; 3rd group - CHD+AH+DM2+obesity. 30 healthy individuals were examined as a control group.All participants underwent a general clinical examination (history, arterial blood pressure, body mass index), standard cardiological examinations (ECG, echocardiography). Within the framework of laboratory studies, the acid-base status (pH, pCO2, HCO3, excess of bases in arterial blood) and hemostasis system parameters (platelet count, APTT, prothrombin time/IRR, fibrinogen, D-dimer) were assessed. Comparative analysis of the obtained data was carried out in the context of groups, correlation analysis between AAB and hemostasis indicators, as well as a multifactorial regression method was used to assess the influence of the degree of comorbidity.
3. Results and Analyses
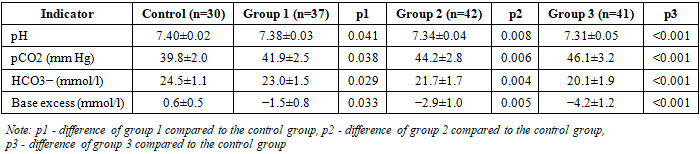
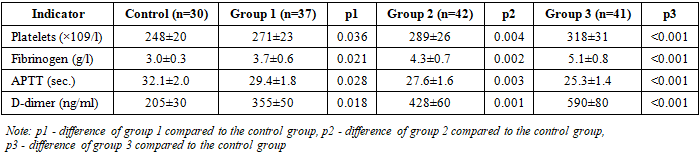
- As comorbid conditions deepened, the clinical course of CHD, changes in the ABB and hemostasis system became more pronounced (Table 1).
|

|
|
|
|
4. Discussion
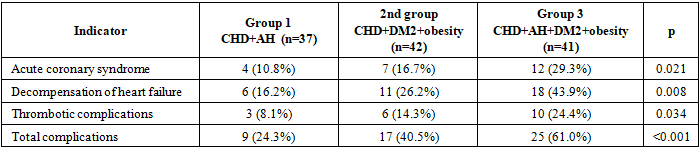
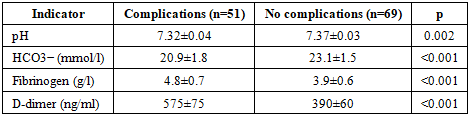
- This study demonstrates that the increasing comorbidity burden in patients with coronary heart disease is associated with progressive metabolic and hemostatic disorders that significantly influence clinical severity and the risk of adverse cardiovascular events. The stepwise deterioration of acid-base balance, particularly the decrease in pH, HCO3−, and base excess values, indicates the development of metabolic acidosis, which became most pronounced in patients with combined arterial hypertension, type 2 diabetes mellitus, and obesity.Metabolic acidosis is not only a biochemical abnormality but also an important pathophysiological factor affecting vascular homeostasis. Even mild chronic acidosis can impair endothelial function, reduce nitric oxide bioavailability, and promote inflammatory activation [2,7,11]. In diabetic and obese patients, tissue hypoxia, insulin resistance, and mitochondrial dysfunction enhance anaerobic metabolism and lactate accumulation, further aggravating acidosis [3]. These mechanisms contribute to vascular instability and coronary microcirculatory disorders.In parallel with ABB disorders, our study revealed a progressive increase in thrombogenic activity. Elevated platelet count, fibrinogen, and D-dimer levels, combined with shortened APTT, reflect the activation of coagulation pathways and hypercoagulable state. It is well established that the structure and density of fibrin clots significantly influence the thrombotic risk [4,6], while elevated D-dimer concentrations are strongly associated with adverse cardiovascular outcomes [5]. A pronounced increase in fibrinogen and D-dimer in the third comorbid group confirms the amplification of thrombin generation and fibrinolytic activity in advanced metabolic dysregulation.Importantly, patients with documented cardiovascular complications demonstrated significantly lower pH and HCO3− values and higher fibrinogen and D-dimer concentrations. These findings suggest that metabolic acidosis and hypercoagulation are not independent phenomena but interconnected components of a unified pathophysiological cascade. Acidosis may enhance platelet aggregation and coagulation factor activation, while systemic inflammation and endothelial dysfunction further accelerate thrombogenesis [2,7,8].The observed increase in acute coronary syndrome, decompensation of heart failure, and thrombotic events with an increasing comorbidity burden supports the concept of the cardio-metabolic continuum [9,10,12]. Combined hypertension, diabetes, and obesity create a hemodynamic and metabolic environment that promotes myocardial remodeling, endothelial damage, and atherothrombosis. Chronic neurohumoral activation and oxidative stress aggravate both myocardial ischemia and systemic prothrombotic state [2,9].Thus, our findings substantiate the pathogenetic link between acid-base imbalance and activation of the hemostasis system in comorbid CHD. The combined assessment of blood pressure parameters and hemostasis biomarkers provides additional prognostic information beyond traditional clinical evaluation. The integration of these laboratory markers into routine cardiological practice may enhance early risk stratification and allow for timely preventive interventions, especially in patients with multiple metabolic comorbidities.Overall, the results confirm that metabolic acidosis and hypercoagulability represent key mechanisms contributing to an unfavorable cardiovascular prognosis in comorbid ischemic heart disease.
5. Conclusions
- The presence of comorbid conditions with coronary heart disease (AH, type 2 DM and obesity) significantly increases the clinical severity of the disease, manifested by an increase in the proportion of functional classes III-IV; at the same time, with an increase in the level of comorbidity, the tendency towards metabolic acidosis in the acid-base state intensifies (pH, HCO3− and base excess significantly decreased), hypercoagulation disorders in the hemostasis system (increased platelets, fibrinogen and D-dimer, decreased APTT) increase, especially in the group of CHD+AH+DM2+obesity (p<0.001), which substantiates the presence of a pathogenetic link between the imbalance of ABB and thrombogenic activity, and the expediency of using these biomarkers in the stratification of clinical risk and early prediction of complications.It was established that the development of adverse cardiovascular complications in comorbid conditions with coronary heart disease is reliably associated with a tendency towards metabolic acidosis and an increase in hypercoagulation: in patients with complications, the pH and HCO3− indicators decreased significantly, while the levels of fibrinogen and D-dimer increased significantly (p≤0.002). In groups with a combination of comorbid factors, the frequency of complications was high, which indicates that the imbalance of the ABB and the activation of the hemostasis system play an important role in the clinical course and prognosis of CHD. Therefore, a comprehensive assessment of these biomarkers can be used as an effective clinical instrument for the early detection of adverse cardiovascular events and risk stratification.