-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1285-1288
doi:10.5923/j.ajmms.20261603.90
Received: Feb. 16, 2026; Accepted: Mar. 12, 2026; Published: Mar. 23, 2026

Review Article: Pathomorphology of Hepatoblastoma- Current Concepts and Clinicopathological Correlation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIshmuratov F. E.1, Madaliev A. A.2, Karimov A. R.3
1Pathomorphologist, Karakalpakstan branch of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
2Head of the Pathomorphology Department of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
3Pathomorphologist, Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

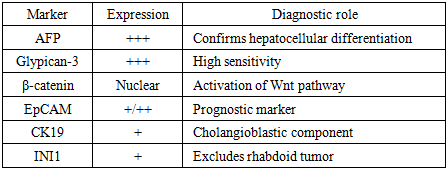
Background: Hepatoblastoma (HB) is the most common primary malignant liver tumor in children, although it remains a rare neoplasm overall. Advances in molecular pathology and immunohistochemistry have significantly improved the understanding of its biological behavior, histological diversity, and clinical management. Objective. This review aims to summarize current knowledge on the pathomorphology of hepatoblastoma, focusing on histological classification, immunohistochemical characteristics, molecular alterations, and their clinicopathological correlations. Methods. A narrative review of recent literature was conducted, analyzing studies on the histopathological features, molecular mechanisms, and diagnostic markers of hepatoblastoma. Particular attention was given to the modern histological classification and standardized pathology reporting systems. Results. Hepatoblastoma demonstrates a broad spectrum of histological patterns, including epithelial, mixed epithelial–mesenchymal, and rare teratoid variants. Key epithelial subtypes include fetal, embryonal, macrotrabecular, cholangioblastic, and small cell undifferentiated forms. Immunohistochemical markers such as Glypican-3, β-catenin, EpCAM, AFP, and CK19 play an essential role in confirming the diagnosis and identifying tumor differentiation patterns. Molecular studies highlight frequent mutations in the CTNNB1 gene and activation of the Wnt/β-catenin signaling pathway, supporting the hypothesis that hepatoblastoma arises from pluripotent hepatic precursor cells. Conclusion: Pathomorphological evaluation remains fundamental for accurate diagnosis and risk stratification in hepatoblastoma. Standardized histological reporting and integration of molecular data may improve prognostic assessment and guide personalized therapeutic strategies for affected patients.
Keywords: Hepatoblastoma, Pediatric liver tumors, Pathomorphology, Immunohistochemistry, Molecular pathology, Wnt/β-catenin pathway, CTNNB1 mutation, Clinicopathological correlation
Cite this paper: Ishmuratov F. E., Madaliev A. A., Karimov A. R., Review Article: Pathomorphology of Hepatoblastoma- Current Concepts and Clinicopathological Correlation, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1285-1288. doi: 10.5923/j.ajmms.20261603.90.
1. Introduction
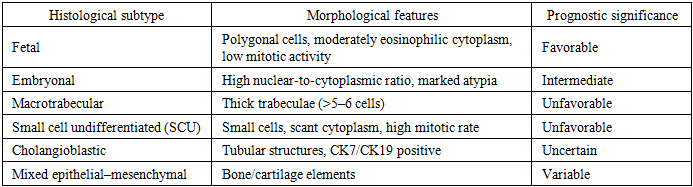
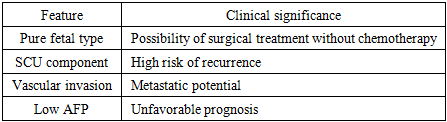
- Hepatoblastoma (HB) is a rare malignant blastomatous tumor of the liver characterized by various combinations of epithelial and mesenchymal cellular lineages that recapitulate early stages of liver ontogenesis. Hepatoblastoma usually occurs in children and is most commonly diagnosed before the age of 5 years, with an incidence of approximately 1.5 cases per million children per year [18]. Very rarely, hepatoblastoma develops in older children and adults.Hepatoblastoma accounts for less than 5% of all malignant tumors in children. The tumor occurs more frequently in children with low birth weight and is associated with several molecular and cytogenetic abnormalities, including frequent mutations in the Wnt/β-catenin signaling pathway [16].Morphologically, hepatoblastomas are divided into epithelial and mixed epithelial–mesenchymal types. Epithelial tumors are further classified into fetal, embryonal, macrotrabecular, and small cell undifferentiated subtypes, whereas mixed epithelial–mesenchymal hepatoblastomas are subdivided into tumors with or without teratoid features. The small cell undifferentiated subtype may demonstrate rhabdoid features associated with loss of expression of the INI1 gene, similar to malignant rhabdoid tumors [11]. Although hepatoblastomas are aggressive tumors with a high rate of recurrence and metastasis, modern treatment approaches provide excellent outcomes. To improve treatment effectiveness, molecular profiling is increasingly used to enable more precise risk stratification.Clinically, the disease usually presents with abdominal enlargement, possible abdominal pain, elevated levels of α-fetoprotein (AFP), and the presence of a solitary hepatic mass [6]. Individuals with familial adenomatous polyposis (FAP)—a syndrome characterized by early development of colorectal polyps and adenocarcinoma—frequently develop hepatoblastoma [8,15]. In addition, mutations in β-catenin are commonly found in sporadic hepatoblastomas, occurring in approximately 67% of patients [12]. Recent studies have shown that other components of the Wnt signaling pathway may also contribute to constitutive pathway activation leading to hepatoblastoma development [14]. Accumulating evidence suggests that hepatoblastoma originates from a pluripotent stem cell [13].Syndromes associated with an increased incidence of hepatoblastoma include:• Beckwith–Wiedemann syndrome• Edwards syndrome• Down syndrome• Aicardi syndrome• Li–Fraumeni syndrome• Goldenhar syndrome• von Gierke disease• familial adenomatous polyposis [9,10]Although hepatoblastoma remains a rare neoplasm, current approaches to its classification and pathomorphological analysis necessitate standardized reporting of biopsy and resection specimens.Histological Classification. The modern classification identifies several major histological types of hepatoblastoma:1. Epithelial type, including:• Fetalo fetal with low mitotic activity (well-differentiated)o mitotically active fetal (“crowded fetal”)o pleomorphic2. Embryonal3. Small cell undifferentiated (SCU)• SMARCB1 (INI1)-negative• SMARCB1 (INI1)-positive4. Cholangioblastic5. Macrotrabecular6. Mixed epithelial–mesenchymal (with or without teratoid elements)The teratoid variant is a rare morphology characterized by elements of neuroectoderm, melanin, and endodermal tissues [17]. Epithelial forms reflect different stages of hepatocyte differentiation: fetal morphology demonstrates features of more mature tissue, whereas embryonal variants represent more primitive structures with a high nuclear-to-cytoplasmic ratio (Fig. 1).
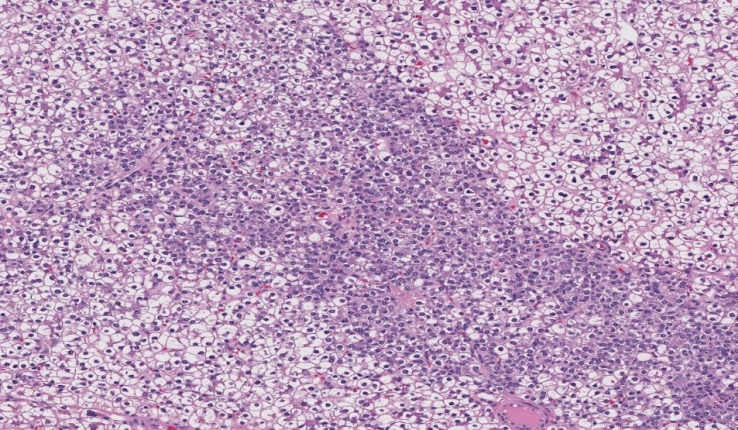 | Figure 1. Epithelial hepatoblastoma, pure fetal type. Alternating light and dark areas are observed; the light areas correspond to hepatoblasts with clear cytoplasm due to the accumulation of glycogen and lipids, which are absent in hepatoblasts forming the darker regions. Magnification ×100, H&E |
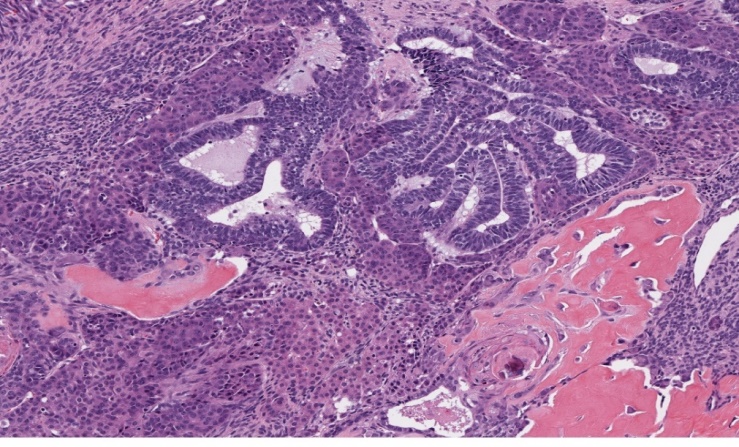 | Figure 2. Mixed epithelial–mesenchymal hepatoblastoma. The tumor contains embryonal and fetal epithelial components intermingled with mesenchymal elements including fibrous, osteoid, and squamous differentiation. Magnification ×100, H&E |
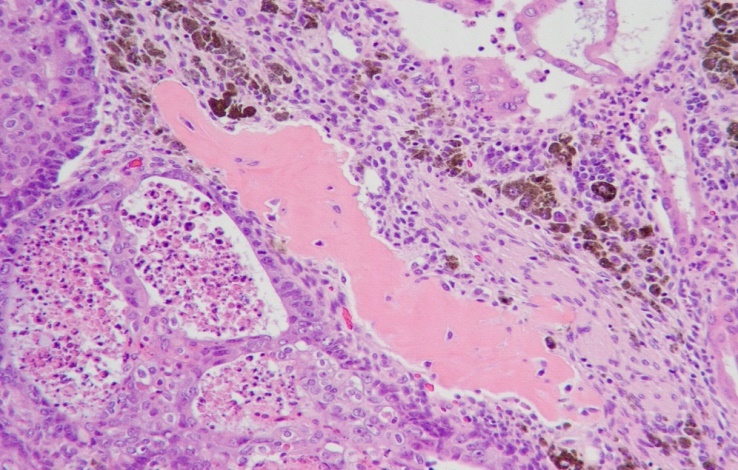 | Figure 3. Mixed epithelial–mesenchymal hepatoblastoma with teratoid features, including embryonal and fetal epithelial components intermingled with osteoid and neural elements containing melanin. Magnification ×100, H&E |
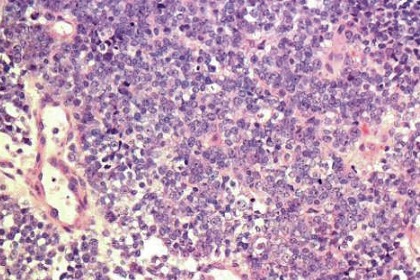 | Figure 4. Small immature cells with an increased nuclear-to-cytoplasmic ratio forming a diffuse growth pattern. Magnification ×100, H&E |
|
|
|
2. Reporting Recommendations
- The International Collaboration on Cancer Reporting (ICCR) recommends including the following parameters in pathology reports for hepatoblastoma:• histological tumor subtype• presence of mesenchymal or teratoid components• degree of differentiation / mitotic activity• immunohistochemical profile• presence of vascular invasion• correlation with clinical and molecular data [5]
3. Conclusions
- Pathomorphological examination of hepatoblastoma is a key component in diagnosis and risk stratification for patients with this rare tumor. Recent international recommendations aim to standardize morphological and immunohistochemical approaches, thereby improving diagnostic accuracy, prognostic assessment, and therapeutic management.