-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1280-1284
doi:10.5923/j.ajmms.20261603.89
Received: Feb. 25, 2026; Accepted: Mar. 15, 2026; Published: Mar. 23, 2026

Organ-Preserving Surgery for Splenic Injuries: Modern Approaches, Minimally invasive Techniques, and Efficacy Analysis (2017–2024)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. A. Khadjiboev, F. Q. Gulomov, M. M. Pulatov, J. N. Juraev, Y. A. Abdurakhmanov
Republican Research Centre of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Splenic injuries remain a significant challenge in emergency abdominal surgery. While splenectomy has traditionally been the standard approach, organ-preserving strategies are increasingly adopted due to the severe consequences of postsplenectomy syndrome. This study aimed to evaluate the efficacy and safety of organ-preserving operations in a retrospective-prospective analysis of 273 patients over 8 years. Methods. A total of 273 patients who underwent surgical treatment for splenic injuries at RSCEMC between 2017 and 2024 were analyzed. Splenectomy was performed in 240 patients (87.9%) and organ-preserving surgery in 33 patients (12.1%). Results. The groups were comparable in age (34.4±13.4 vs 31.9±11.1 years; p=0.239) and sex (male 59.2% vs 54.5%; p=0.751). Organ-preserving operations achieved 100% success in AAST grade I–III injuries (33/33). Mortality was 0% in the organ-preserving group versus 18.3% in the splenectomy group (p=0.004). Laparoscopic approach was used in 13 cases (39.4%). Hospital stay was 11.8±8.9 vs 12.2±13.4 days (p=0.814). Conclusion. Organ-preserving operations are safe and effective in selected patients: 100% success rate, 0% mortality, and 0% conversion. Laparoscopic techniques further expand the possibilities of splenic preservation.
Keywords: Splenic injury, Organ-preserving surgery, Splenectomy, Laparoscopy, AAST, Hemostasis, Overwhelming postsplenectomy infection (OPSI)
Cite this paper: F. A. Khadjiboev, F. Q. Gulomov, M. M. Pulatov, J. N. Juraev, Y. A. Abdurakhmanov, Organ-Preserving Surgery for Splenic Injuries: Modern Approaches, Minimally invasive Techniques, and Efficacy Analysis (2017–2024), American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1280-1284. doi: 10.5923/j.ajmms.20261603.89.
Article Outline
1. Introduction
- Splenic injuries are among the most common and clinically significant conditions in emergency abdominal surgery. The spleen is the most frequently injured parenchymal organ in blunt abdominal trauma, accounting for 16–30% of all blunt abdominal injuries [1,2]. In polytrauma cases, this rate increases to 49% [3], with concurrent injuries to other abdominal and retroperitoneal organs observed in up to 70% of cases [4].For decades, splenectomy was the standard surgical approach for splenic injuries. However, the growing recognition of the spleen’s critical role in the immune system led to a paradigm shift in surgical strategy [6,7]. Postsplenectomy syndrome (OPSI) is characterized by increased susceptibility to severe infections caused by encapsulated organisms such as Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis. The lifetime risk of OPSI is 5%, with mortality rates of 50–70% once established [8,9].Modern hemostasis technologies electrocoagulation, argon plasma coagulation (APC), and hemostatic agents have expanded the scope of organ-preserving approaches [10,11]. Laparoscopic surgery has further enhanced the possibilities for splenic preservation [12,13]. The American Association for the Surgery of Trauma (AAST) classification standardizes injuries from grade I to V [14]. Current evidence suggests that nonoperative management can be successful in up to 90% of hemodynamically stable patients [15].Data on organ-preserving approaches for splenic injuries from Central Asian countries remain scarce. This study presents the first comprehensive 8-year experience from a high-volume emergency surgical center in Uzbekistan.
2. Study Aim
- The primary aim was to evaluate the efficacy and safety of organ-preserving operations for splenic injuries and compare outcomes with splenectomy. Secondary aims included identifying optimal patient selection criteria and evaluating the role of laparoscopic techniques.
3. Materials and Methods
3.1. Study Design
- This was a combined retrospective-prospective observational study conducted at RSCEMC, Tashkent, Uzbekistan. A total of 273 patients who underwent surgical treatment for splenic injuries between 2017 and 2024 were included.
3.2. Ethical Approval
- The study was approved by the Institutional Ethics Committee of RSCEMC. All procedures were conducted in accordance with the Declaration of Helsinki.
3.3. Patients
- Inclusion criteria: age ≥18 years, confirmed splenic injury, requirement for surgical intervention. Exclusion criteria: nonoperative management, incomplete medical records, iatrogenic splenic injuries.
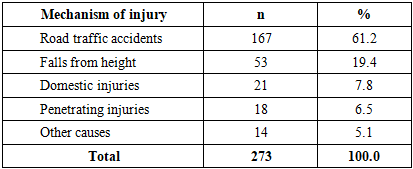
3.4. Demographics
- The mean age was 34.1 years (range: 18–83), with 160 males (58.6%) and 113 females (41.4%). The distribution of injury mechanisms is presented in Table 1.
|
3.5. Diagnostic Workup
- All patients were assessed per the ATLS protocol. FAST ultrasonography was performed to detect free intraperitoneal fluid. Hemodynamically stable patients underwent contrast-enhanced CT. Splenic injuries were graded according to the AAST Organ Injury Scale [14].
3.6. Surgical Techniques
- Splenectomy was performed via open midline laparotomy. Organ-preserving operations were performed via open or laparoscopic approach. Hemostatic techniques included bipolar electrocoagulation, argon plasma coagulation (APC), and hemostatic sponges. Patient selection criteria for organ preservation: hemodynamic stability, AAST grade I–II injury, hemoperitoneum <500 mL.
3.7. Statistical Analysis
- Descriptive statistics were used. Continuous variables are presented as mean±SD; categorical variables as n (%). Comparisons were performed using Student’s t-test, χ² test, and Fisher’s exact test. p<0.05 was considered statistically significant.
4. Results
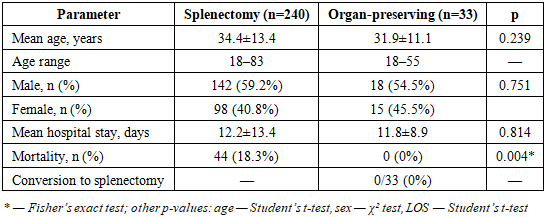
4.1. Overall Outcomes
- Of 273 patients, 240 (87.9%) underwent splenectomy and 33 (12.1%) underwent organ-preserving operations. In none of the organ-preserving cases (0/33) was conversion to splenectomy required. The two groups were comparable in age (p=0.239) and sex distribution (p=0.751) (Table 2).
|
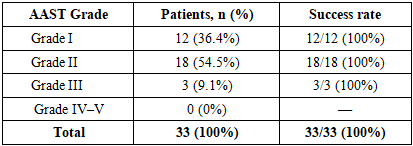
4.2. AAST Grade-Based Outcomes
- Organ-preserving operations achieved a 100% success rate in AAST grade I–II injuries (30/30). All 3 patients with grade III injuries were also managed successfully. No organ-preserving surgery was attempted in grade IV–V injuries (Table 3).
|
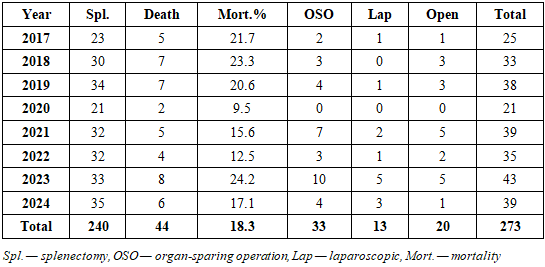
4.3. Temporal Trends
- The proportion of organ-preserving operations increased from 8.0% (2/25) in 2017 to 23.3% (10/43) in 2023. Laparoscopic cases rose from 1 in 2017 to 8 in 2023–2024. No organ-preserving surgery was performed in 2020 (pandemic year). Overall splenectomy mortality was 18.3% (Table 4).
|
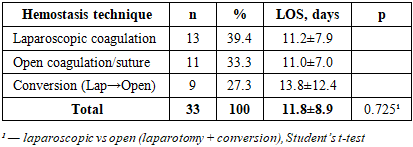
4.4. Organ-Preserving Techniques
- Of the 33 organ-preserving operations, 13 (39.4%) were performed laparoscopically, 11 (33.3%) via open coagulation/suture repair, and 9 (27.3%) required conversion from laparoscopy to laparotomy. Hospital stay did not differ significantly between laparoscopic and open approaches (11.2 vs 12.2 days, p=0.725) (Table 5).
|
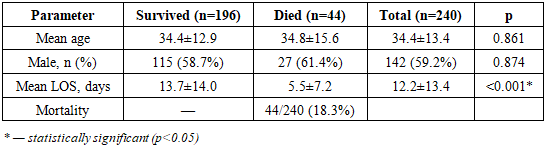
4.5. Mortality Analysis in the Splenectomy Group
- Of 240 splenectomy patients, 44 (18.3%) died. The majority of deceased patients had severe concomitant injuries (traumatic brain injury, polytrauma). Hospital stay among non-survivors was significantly shorter than among survivors (5.5±7.2 vs 13.7±14.0 days; p<0.001), indicating early mortality (Table 6).
|
4.6. Complications
- No spleen-related postoperative complications were observed in the organ-preserving group (0/33, 0%): no rebleeding, subdiaphragmatic abscess, or wound infection. One patient (3.0%) required neurosurgical reoperation for rebleeding from a concomitant craniocerebral injury (unrelated to the splenic procedure).
5. Discussion
- Our findings contribute to the growing evidence base supporting organ-preserving approaches for splenic injuries. The overall organ preservation rate of 12.1% (33/273) is consistent with reports from comparable emergency surgical settings, though lower than the 60–90% nonoperative management rates reported by specialized trauma centers in high-income countries [17,18]. This disparity is likely attributable to delayed presentation, higher prevalence of polytrauma, and the unavailability of splenic artery embolization (SAE) at our institution during the study period.The 100% success rate in AAST grade I–II injuries (30/30) validates our patient selection criteria. The absence of spleen-related complications and reoperations (0/33) confirms the safety of this approach. The successful management of all 3 grade III cases (3/3) demonstrates cautious expansion of indications [19,20]. No organ-preserving surgery was attempted in grade IV–V injuries, consistent with international guidelines recommending splenectomy for hemodynamically unstable patients with high-grade injuries.The two groups showed no statistically significant differences in age (p=0.239), sex (p=0.751), or hospital stay (p=0.814). However, the mortality difference was highly significant (0% vs 18.3%, p=0.004). This finding should be interpreted with caution given the inherent selection bias (confounding by indication): organ-preserving candidates were by definition hemodynamically stable with lower-grade injuries.The synergistic use of APC, bipolar electrocoagulation, and hemostatic sponges was critical for achieving definitive hemostasis [21,22]. The conversion rate of 27.3% is within the internationally reported range of 20–35% and was attributable to intraoperative findings of more extensive injury than anticipated.The progressive adoption of laparoscopic techniques (from 1 case in 2017 to 8 in 2023–2024) reflects the institutional learning curve. The overall laparoscopic rate of 39.4% demonstrates feasibility in the emergency setting with appropriate training [25,26].The predominance of road traffic accidents (61.2%) is consistent with the epidemiology of the Central Asian region [28,29]. The relatively young mean age (34.1 years) underscores the socioeconomic impact of splenic injuries on the working-age population.Limitations: 1) retrospective component with inherent biases; 2) selection bias (confounding by indication); 3) small sample size in the organ-preserving group (n=33); 4) absence of standardized injury severity scoring (ISS); 5) lack of long-term immunological follow-up data. Future prospective studies with standardized protocols will strengthen the evidence base.
6. Conclusions
- 1. Organ-preserving operations for splenic injuries demonstrated 100% success in AAST grade I–III injuries (33/33), with 0% mortality and 0% conversion to splenectomy (p=0.004 vs splenectomy group).2. Over the 8-year period, the proportion of organ-preserving operations increased from 8.0% to 23.3%, with laparoscopic utilization reaching 39.4%.3. Splenectomy mortality was 18.3% (44/240), with significantly shorter hospital stay among non-survivors (5.5 vs 13.7 days, p<0.001) indicating early mortality.4. Key criteria for successful splenic preservation include: hemodynamic stability, hemoperitoneum ≤500 mL, AAST grade I–II injury, and absence of severe concomitant abdominal injuries.5. Future directions should include implementation of SAE, cautious expansion of indications to grade III injuries, and evaluation of long-term immunological outcomes.