-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1142-1150
doi:10.5923/j.ajmms.20261603.61
Received: Feb. 8, 2026; Accepted: Mar. 3, 2026; Published: Mar. 13, 2026

Effectiveness of Stress Inoculation Therapy (SIT) in the Mitigation of Posttraumatic Stress Disorder (PTSD) Among Frontline Nigerian Army Personnel in North-West Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdebayo David Oluwole 1, Adeyinka Abideen Aderinto 2, Oyesoji Aremu 1, Adedeji Tella 3, Olarenwaju A. Oladejo 4, Farida Abubakar 5, Jamilah Musa 6, Hadizan Usman 7
1Department of Counselling and Human Development Studies, University of Ibadan, Nigeria
2Department of Sociology, University of Ibadan, Nigeria
3Department of Science and Technology Education, University of Ibadan, Nigeria
4Department of Peace, Security and Humanitarian Studies, University of Ibadan, Nigeria
5Department of Sociology, Umaru Musa Yar'adua University, Katsina, Nigeria
6Department of Sociology, Sule Lamido University, Kafin Hausa, Jigawa State, Nigeria
7Department of Sociology, Gombe State University, Gombe, Nigeria
Correspondence to: Adebayo David Oluwole , Department of Counselling and Human Development Studies, University of Ibadan, Nigeria.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study was designed to investigate the effectiveness of stress inoculation therapy (SIT) in the mitigation of posttraumatic stress disorder (PTSD) among frontline Nigerian Army personnel in North-West Nigeria. Employing a mixed-methods design, a total of 38 personnel from 1 Division of the Nigerian Army, Kaduna diagnosed with PTSD were purposively selected to participate in the study, with the majority being young (63.2%) and male (73.6%). Data were collected using the PTSD Assessment Tool (PSS-I-5) and the Combat Exposure Scale (CES), and analysed using frequency counts, percentages, and t-tests. Results indicated a significant reduction in PTSD symptoms following SIT (t (74) = 3.671, p < .05), confirming its effectiveness. No significant differences were observed in posttest PTSD scores based on gender (t (36) = -1.090, p = .283) or age (t (36) = 0.930, p = .359). These findings suggest that SIT is effective in mitigating PTSD among combat-exposed army personnel, irrespective of age or gender. The study highlights the importance of targeted psychological interventions for frontline military personnel to enhance resilience and reduce the recurrence of trauma-related symptoms.
Keywords: Posttraumatic stress disorder, Nigerian Army, Stress inoculation therapy, Frontline personnel, Psychological intervention
Cite this paper: Adebayo David Oluwole , Adeyinka Abideen Aderinto , Oyesoji Aremu , Adedeji Tella , Olarenwaju A. Oladejo , Farida Abubakar , Jamilah Musa , Hadizan Usman , Effectiveness of Stress Inoculation Therapy (SIT) in the Mitigation of Posttraumatic Stress Disorder (PTSD) Among Frontline Nigerian Army Personnel in North-West Nigeria, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1142-1150. doi: 10.5923/j.ajmms.20261603.61.
Article Outline
1. Introduction
- Nigeria, Africa's most populous nation and largest economy, has grappled with diverse security threats, including terrorism, insurgency, banditry, kidnapping, communal clashes, and herders–farmers conflicts. The emergence of Boko Haram opened the floodgate for other terror groups such as the Islamic State of West African Province (ISWAP), which operates in the northeast, and Lakuruwa in the northwest region of the country. In the north-central region, security threats include banditry, farmer–herder clashes and Fulani jihadist groups. A new group that recently ravaged the north-central region is known as Mahmudah [1].Exposure to traumatic life events can lead to a wide range of significant and enduring psychological consequences. Over the past three decades, scholarly work on trauma and its mental health effects has grown substantially, with posttraumatic stress disorder (PTSD) becoming one of the most extensively examined outcomes among survivors of violence, conflict, and large-scale disasters [2,3]. Epidemiological investigations consistently identify PTSD as one of the most commonly studied mental health conditions among trauma-exposed populations [4].Frontline Nigerian soldiers frequently face persistent fear and anxiety, including fear of death, fear of killing innocent persons, and anticipatory fear linked to unpredictable combat environments. When these reactions become prolonged, exaggerated, or disruptive, they can escalate into pathological levels of psychological distress and mental health challenges. The problem is further compounded by the chronic operational overstretch of Nigerian military personnel. Many soldiers spend extended periods—sometimes months or years—away from home, only to be redeployed shortly after returning from theatres of operation. This cycle of repeated exposure to high-intensity conflict and cumulative stressors places them at increased risk of psychological breakdown, diminished operational readiness, and long-term mental health complications.This study, therefore, seeks to assess the impact of Stress Inoculation Therapy (SIT) on PTSD among frontline Nigerian Army personnel in Nigeria in improving psychological outcomes. Addressing this gap is essential for enhancing soldiers’ wellbeing, improving military readiness, and strengthening the psychosocial support structures within the Nigerian Armed Forces. Specifically, the study determined the effect of Stress Inoculation Therapy (SIT) on PTSD levels among frontline Nigerian Army personnel by comparing their pretest and posttest PTSD scores. It also examined gender differences in posttest PTSD scores among frontline Nigerian Army personnel exposed to Stress Inoculation Therapy, as well as investigated age-related differences in posttest PTSD scores among frontline Nigerian Army personnel exposed to Stress Inoculation Therapy.This study is anchored in Jones and Barlow’s Anxious Apprehension Model, which provides a relevant perspective for understanding posttraumatic stress disorder (PTSD) among frontline military personnel. According to Jones and Barlow, mechanisms implicated in panic disorder are also central to the development and maintenance of PTSD. Specifically, there are marked parallels between panic attacks and traumatic flashbacks [5].In PTSD, anxious apprehension is directed toward cognitive and physiological cues reminiscent of the trauma. The resulting hyperarousal symptoms (e.g., heightened startle response, irritability, concentration difficulties) are reinforced through a negative feedback loop, which maintains re-experiencing symptoms such as flashbacks and intrusive memories. To manage the distress from these alarms, affected individuals may engage in avoidance behaviours—both internal (emotional numbing) and external (avoiding trauma-related stimuli). Jones and Barlow further argue that coping styles and social support can moderate the severity and expression of PTSD, similar to their effects in other anxiety disorders [5].The Anxious Apprehension Model has been applied in several studies. For instance, it has been used to examine anxiety and PTSD among individuals exposed to violence [6]. Similarly, Warren et al. investigated adults experiencing a range of anxiety and depressive symptoms using resting-state functional magnetic resonance imaging (fMRI) within the framework of the anxious apprehension model [7]. In the present study, this model underscores how Stress Inoculation Therapy (SIT) can be theoretically justified: by enhancing coping mechanisms, reducing hypervigilance, and restructuring maladaptive cognitive appraisals, such interventions may disrupt the negative feedback loop and reduce PTSD symptoms among frontline military personnel.
2. Materials and Methods
2.1. Research Design
- This study adopted a single-case quasi-experimental design to investigate the effectiveness of Stress Inoculation Therapy (SIT) in mitigating PTSD symptoms and preventing recurrence among affected personnel. Single-case quasi-experimental designs are commonly used when random assignment of participants to treatment and control groups is not feasible, yet the researchers seek to establish causal inferences through repeated measurement, systematic observation, and controlled manipulation of variables. In this study, the frontline army personnel who were experiencing PTSD within the Nigerian Army were compared without random assignment. The design enabled the researchers to assess changes in the outcome variable (PTSD) as influenced by SIT intervention, age and gender factors, while accounting for pre-existing group characteristics. This approach is appropriate for military operational setting where intervention or random assignment is impractical.
2.2. Sample and Sampling
- The participants consisted of Nigerian Army personnel who had been diagnosed with PTSD in North-West Nigeria. A complete enumeration approach was used, targeting all personnel who met the inclusion criteria within the study location. All participants received SIT intervention at the Division 1 of the Nigerian Army in Kaduna for eight weeks.
2.3. Sample Profile
- The socio-demographic data indicate that the majority of participants were young frontline personnel, with 24 individuals (63.2%) classified as “young” and 14 (36.8%) as “old.” Age ranged from 20 to 41 years and above, with the largest subgroup being 20–25 years (50%). The mean age of participants was 32.32 ± 11.76 years. In terms of gender, 28 participants (73.6%) were male, while 10 (26.3%) were female.
2.4. Procedure for Data Collection
- Data collection was conducted directly within military environment to ensure access to frontline personnel. Participation was voluntary, and only personnel who provided informed consent were given questionnaires to complete. Efforts were made to create a supportive and flexible environment during data collection to maximize response rates. Researchers employed conversational engagement, encouragement, and reinforcement of participants’ efforts to ensure accurate self-reporting.Using The PTSD Assessment scale, a purposive sampling technique was applied to select participants from different units, focusing exclusively on soldiers with combat operational experience. This approach was appropriate given the study’s emphasis on a specialized population not commonly found in general military samples. The Combat Exposure Scale (CES) was self-administered to collect pretest and posttest data, with researchers providing guidance as needed while respecting participants’ autonomy and confidentiality.
2.5. Instruments
- Combat Exposure Scale (CES)The Combat Exposure Scale (CES) developed by (8) is a 7-item self-report measure that assesses wartime stressors experienced by combatants. Items were rated on a 5-point frequency scale (1 = “no” or “never” to 5 = “more than 50 times”), a 5-point duration scale (1 = “never” to 5 = “more than 6 months”), a 4-point frequency scale (1 = “no” to 4 = “more than 12 times”), or a 4-point degree-of-loss scale (1 = “no one” to 4 = “more than 50%”). The participants indicated their exposures to various combat situations, such as firing at the enemy or performing dangerous duty. Total CES scores (range 0–41) were computed by summing weighted item scores, which were classified into five categories of combat exposure ranging from “light” to “heavy.” The CES was designed to be easily administered and scored, and has been widely used in research and clinical contexts (U.S. Department of Veterans Affairs, 2016). In the original validation, the mean CES score was 25.57 (SD = 10.12), with scores ranging from 1 to 41. Internal consistency was strong, with a coefficient alpha of .85. Item-remainder correlations averaged .75 (range = .64–.83), indicating that the items measured a closely related construct.PTSD Assessment Tool (PSS-I-5)The PTSD Symptom Scale – Interview Version for DSM-5 (PSS-I-5) is a 24-item semi-structured interview used to assess PTSD symptoms experienced in the past month and to determine diagnostic status based on DSM-5 criteria. The interview began with a Criterion A trauma screen and identification of an index trauma when multiple events were reported. Items assessed the frequency and intensity of the 20 DSM-5 PTSD symptoms, while four additional items measured distress, functional interference, onset, and duration. Symptom items were rated on a 5-point scale from 0 (not at all) to 4 (six or more times a week/severe). Symptoms were considered present when rated 1 or higher. The 20 symptom items were summed to generate a total PTSD severity score ranging from 0 to 80. Consistent with DSM-5 criteria, a PTSD diagnosis required the presence of at least one intrusion symptom, one avoidance symptom, two negative alterations in cognition and mood, two arousal symptoms, and clinically significant distress or impairment, operationalised as a score of 2 or above on the relevant items.Internal consistency was strong, with a coefficient alpha of 0.73. This indicated that the instrument is valid.
2.6. The Scientific Procedure
- The study procedures were approved by the Institutional Review Board at the University of Ibadan. The participants completed an intake assessment, which included a semi-structured biopsychosocial interview, administration of the Combat Exposure Scale (CES) to assess for PTSD. The participants were accepted into the program if they were diagnosed with PTSD. Exclusionary criteria included: psychiatric hospitalization within 30 days; suicide or homicide attempt within 30 days; untreated and/or active symptoms of mania or psychosis; untreated and/or active substance use disorders; inability to independently complete activities of daily living; or unstable housing.The intervention was centered on Stress Inoculation Therapy and participants received 45 minutes of weekly sessions for a total of eight [8] sessions. This includes individual and group therapy on trauma-focused counselling and mindfulness. From intake to treatment completion, the soldiers were granted permission to participate by the Nigerian Army.The Stress Inoculation Therapy (SIT) programme used in this study was implemented as a structured, ten-session intervention designed to reduce post-traumatic stress symptoms among frontline Nigerian Army personnel. The training guide provided a systematic sequence of psycho education, cognitive restructuring, coping-skills acquisition, behavioural rehearsal, and practice under gradually increasing stress conditions. Each session built on the previous one to facilitate long-term coping competence.Session 1: Orientation and Pre-Test Administration; Psychoeducation on Stress and CopingThe participants were introduced to the purpose, structure, and expectations of the SIT programme. The pre-test instruments were administered to obtain baseline PTSD and related psychological measures. The participants were taught the transactional model of emotional stress and coping. The session also covered the emotional stress associated with grief and combat-related traumatic experiences, enhancing participants’ understanding of how stress responses are triggered and maintained.Session 2: Introduction to Stress Inoculation TherapyThe stages, theoretical foundations, and therapeutic goals of SIT were explained. The participants were introduced to the concept of “stress vaccination,” which involves building psychological resilience before, during, and after exposure to stressors.Session 3: Self-Monitoring TrainingThe participants were trained to identify and monitor their maladaptive thoughts, images, emotions, and behaviours. This session focused on increasing self-awareness of negative automatic thoughts and trauma-related triggers.Session 4: Cognitive Problem-SolvingThe participants engaged in discussions involving problem definition, consequence-based problem solving, anticipation of stressful situations, decision-making, and evaluating feedback. The aim was to enhance cognitive appraisal and improve adaptive coping strategies.Session 5: Modelling of Coping SkillsDirect-action coping, emotion-regulation strategies, and self-control techniques were demonstrated and practised. Facilitators modelled effective coping behaviours, after which participants engaged in guided practice.Session 6: Cognitive Restructuring Through Self-TalkThe participants were trained to use positive and rational self-talk to counteract maladaptive thoughts. Maladaptive responses were reframed as cues for activating coping strategies rather than as triggers of distress.Session 7: Behavioural Activation I – Mental and Behavioural RehearsalThis session involved practising learned coping strategies through mental rehearsal, role-playing, and controlled simulations. The participants rehearsed behavioural responses to anticipated stressful or trauma-related situations.Session 8: Behavioural Activation II – Graduated Exposure and Skill Reinforcement; Post-Test Administration and Programme Conclusion The participants practised their coping skills in progressively more challenging simulated scenarios to build competence and confidence. Assignments were graded from simple to complex, enabling participants to internalise the use of coping strategies in real-life conditions. The post-test instruments were administered to assess changes in PTSD symptoms and coping abilities. The session also included a summary of the intervention, feedback from participants, and scheduled follow-up procedures.
2.7. Ethical Considerations
- Ethical approval for the study was obtained from the University of Ibadan Ethical Review Committee for Social Sciences and Humanities (UI/SSHREC/2023/00123). Permission was also sought from the Nigerian Army authorities to facilitate informed consent from the participants. The purpose of the study was clearly explained to all the participants, and they were assured that their responses would be treated with the utmost confidentiality. Strict adherence to privacy and protection of participants’ personal information was maintained throughout the study. Participation was entirely voluntary, and only those who provided informed consent completed the questionnaires. The questionnaires were administered through clinicians acting as research collaborators in the Division Hospital and its area of responsibility. The participants were given 60 minutes to complete the questionnaires, after which they were collected. Following data collection, participants identified for the study underwent the psychological interventions.
2.8. Method of Data Analysis
- Data collected from the participants were analysed using both descriptive and inferential statistics. Descriptive statistics, including frequency counts, percentages, means, and standard deviations, were used to summarise the socio-demographic characteristics of the participants and to provide an overview of PTSD scores before and after intervention. Inferential statistics were employed to test the study hypotheses. Paired-samples t-tests were conducted to determine whether there was a significant difference between pretest and posttest PTSD scores of participants exposed to Stress Inoculation Therapy (SIT). Independent-samples t-tests were used to examine potential differences in posttest PTSD scores based on gender and age groups. The t-test is a parametric test that assumes the data follows a normal distribution (or close to it) to be strictly valid. However, due to the Central Limit Theorem (CLT), the t-test is quite robust to non-normal data if the sample size is large (typically n>30 or 50). The level of statistical significance was set at p < .05. All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 25, ensuring accuracy and reliability in reporting the outcomes of the interventions. Results were interpreted in the context of the effectiveness of SIT in mitigating PTSD symptoms among frontline Nigerian Army personnel.
3. Results
- This section presents the result of the study.
3.1. Test of Normality
- Prior to hypothesis testing, the assumption of normality was examined using skewness and kurtosis statistics. According to George and Mallery (2010), values of skewness and kurtosis between −2 and +2 are considered acceptable for establishing normal univariate distribution. Similarly, Hair et al. (2010) and Byrne (2010) suggested that data are normally distributed when skewness values fall between −2 and +2 and kurtosis values fall between −7 and +7. Figure 1 and Figure 2 present the histogram and Q-Q plot of PTSD scores, which further support the assumption of normality are provided as follow:
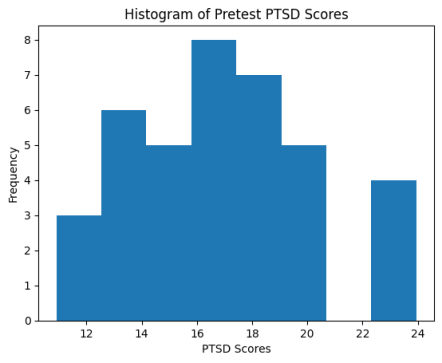 | Figure 1. Histogram of Pretest PTSD Scores |
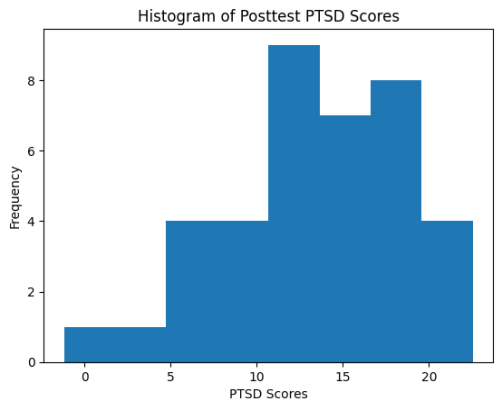 | Figure 2. Histogram of Posttest PTSD Scores |
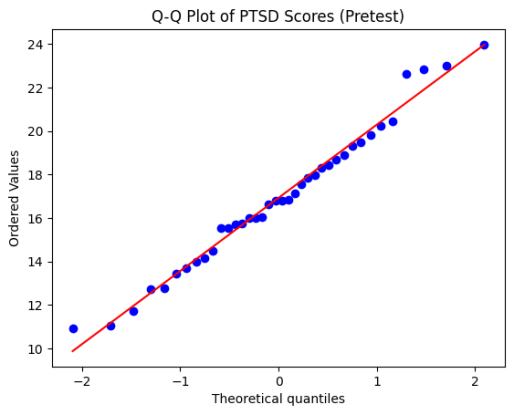 | Figure 3. Normal Q-Q Plot of PTSD Scores |
3.2. Hypothesis 1
- There is no significant difference in pretest and posttest scores of PTSD of frontline Nigerian Army personnel exposed to stress inoculation therapy.
|

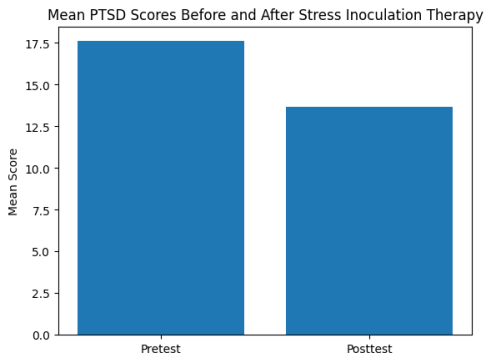 | Figure 4. Mean PTSD Scores Before and After Stress Inoculation Therapy |
3.3. Hypothesis 2
- There is no significant difference in posttest mean scores of PTSD among male and female frontline Nigerian Army personnel exposed to stress inoculation therapy.
|

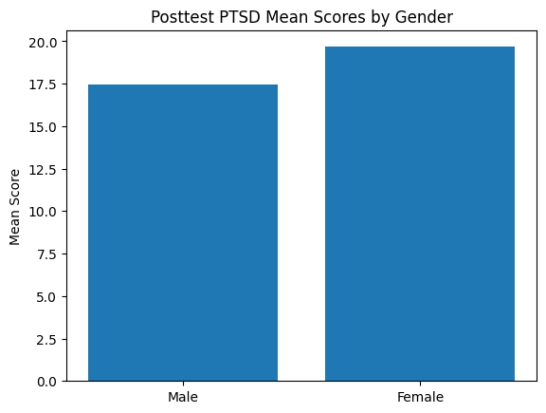 | Figure 5. Posttest PTSD Mean Scores by Gender |
3.4. Hypothesis 3
- There is no significant difference in posttest mean scores of PTSD among young and old frontline Nigerian Army personnel exposed to stress inoculation therapy.
|

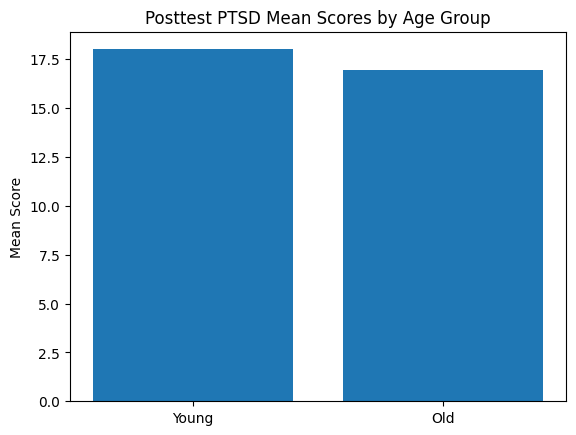 | Figure 6. Posttest PTSD Mean Scores by Age Group |
4. Discussion of Findings
- Effect of Stress Inoculation Therapy on PTSD SymptomsFindings from the study revealed a significant reduction in PTSD symptoms among the participants who underwent Stress Inoculation Therapy. The comparison of pretest and posttest scores indicated that SIT was effective in reducing hyperarousal, intrusive thoughts, avoidance behaviours, and other hallmark symptoms of PTSD among Nigerian Army personnel engaged in frontline operations.This outcome supports earlier studies which demonstrated that SIT is a reliable cognitive–behavioural intervention for trauma-related conditions. Bronson emphasised that SIT works by equipping individuals with coping skills before or after exposure to traumatic events, thereby increasing psychological resilience [9]. Similarly, Etingen, Grubbs and Harik found that cognitive-behavioural interventions significantly reduce PTSD severity [10]. The present study aligns with these findings and extends them to the Nigerian Army context, where prolonged exposure to insurgency, counterterrorism operations, and armed conflict increases vulnerability to trauma.Furthermore, empirical research has explored the effectiveness of Stress Inoculation Training (SIT) in reducing or preventing PTSD among military personnel. Hourani et al. conducted a longitudinal randomized controlled trial with active-duty soldiers and found that SIT did not significantly reduce overall PTSD symptoms or perceived stress when demographic and psychological factors were controlled. However, the intervention demonstrated preventive benefits for soldiers without pre-existing mental health conditions, particularly in reducing hyperarousal symptoms over time [11]. In another study, Jackson et al. reported that veterans who participated in a 12-week group-based SIT program demonstrated significant reductions in PTSD symptoms alongside improvements in perceived knowledge, coping abilities and stress-management performance [12]. Physiological indicators also supported these outcomes, as reduced heart rates during exercises suggested lower stress responses.The improvement observed in the current study suggests that SIT is both culturally adaptable and operationally relevant. Nigerian Army personnel often operate in high-threat environments with limited access to psychological services during deployment. The success of SIT underscores its potential as a structured, scalable and skill-based therapeutic approach suitable for military mental health programmes in Nigeria.Gender Differences in Posttest PTSD LevelsThe study found no statistically significant gender differences in posttest PTSD scores among personnel who received SIT. This suggests that both male and female soldiers benefited equally from the therapeutic intervention. Previous research indicates that early post-trauma manifestations of PTSD symptoms may differ by gender. For instance, women have been found to report higher levels of re-experiencing symptoms and heightened physiological reactivity within one month of exposure to a traumatic event, particularly when confronted with trauma reminders or during recollection of the event, compared with men [13].However, findings from studies employing PTSD symptom network analyses have been mixed with respect to sex- and gender-related differences and have largely overlooked symptom interrelationships during the early post-trauma period. Two studies examining adult populations reported comparable patterns of symptom associations—including symptoms identified as most central within PTSD networks—among women and men [14,15].In contrast, research involving disaster-exposed adolescents with clinically significant PTSD symptoms demonstrated notable gender differences. Cao et al. found that girls exhibited stronger overall connectivity within PTSD symptom networks than boys. Furthermore, gender-specific patterns emerged in the centrality of symptoms: intrusions, flashbacks, avoidance and emotional detachment were more central among girls, whereas flashbacks, psychological cue reactivity, diminished interest and a sense of a foreshortened future were more central among boys [15].Within the context of the Nigerian Army, structured training, comparable combat exposure and strong unit cohesion may mitigate typical gender-related differences in psychological outcomes. Moreover, Stress Inoculation Training (SIT) focuses on universal coping strategies—such as cognitive restructuring, relaxation techniques and problem-solving—that are equally accessible and effective for both men and women.These findings have important implications for policy and programme design, suggesting that gender-specific adaptations of SIT may not be necessary for frontline personnel when operational stressors are largely similar. Universal interventions that strengthen coping skills and resilience can therefore be applied across genders without compromising efficacy.Age-Related Differences in Posttest PTSD ScoresThe study also showed no significant age-related differences in posttest PTSD levels among treated personnel. This indicates that SIT was effective across age categories and that age did not moderate therapeutic improvement. The present finding corroborates that of Gielkens et al., who compared the effectiveness of an intensive trauma-focused treatment programme on PTSD symptom severity in older and younger adults. Their results showed substantial reductions in PTSD symptoms across both age groups following treatment, with older adults benefiting just as much as younger adults [16].Although many studies have investigated age differences in PTSD symptoms, results remain inconclusive. For instance, Pietrzak et al. reported that older adults exposed to trauma may show different symptom patterns and coping responses compared with younger adults, but overall prevalence and severity patterns remain inconsistent across studies [17]. Similarly, Bonanno et al. observed considerable variability in trauma responses across age groups, with resilience and recovery patterns influenced more by individual and contextual factors than by chronological age alone [18].One reason for these mixed findings may be that studies have examined victims of different trauma types and assessed them at varying intervals after trauma exposure—from immediately after the event to several decades later. Such methodological differences may contribute to inconsistent findings regarding age-related PTSD patterns.The coping strategies taught in SIT—such as relaxation techniques, systematic desensitization and cognitive reframing—are largely age-neutral and do not depend heavily on developmental stage. This may explain why participants across age categories in the present study experienced similar therapeutic benefits.This outcome further reinforces the adaptability and broad applicability of SIT within diverse military settings, making it an effective component of psychological support programmes for personnel of varying age groups.
5. Limitations of the Study
- Despite the valuable insights provided by this study on the effectiveness of stress inoculation therapy in reducing post-traumatic stress disorder (PTSD) among frontline Nigerian Army personnel, it is important to acknowledge a number of potential drawbacks.First, the sample population for this study is quite small (N = 38), and this could have a bearing on whether its outcomes can be generalized to Nigerian Army Personnel at large or even beyond other military populations. A larger sample would have given much of a sample to give strength to the statistic and confirm the generalizability of the findings.Secondly, the study is also faced with another limitation in that it restricted the sample to a singly perceived military population, frontlines of the Nigerian Army. Hence the findings cannot be generalized to other service branches, such as the navy, air force, or non-military populations having historically been exposed to traumatic occurrences.Third, the research had a pretest-posttest design which limits casual inference for the observed decrease in PTSD symptoms solely to stress inoculation therapy. Environmental factors, coping behaviors, or social systems might have all contributed to the observed changes.Fourthly, in the sample skewing the gender balance, the significant difference in the distribution of female to male participants might have likewise had an influence on any potentially detected gender characteristics of PTSD manifestations. Finally, the major emphasis of the study was put on the short-term effects of stress inoculation treatment. It is now necessary for longitudinal studies to determine the stability of post-traumatic stress symptoms over time.
6. Conclusions
- The findings of this study demonstrate that Stress Inoculation Training (SIT) is an effective intervention for reducing PTSD symptoms among frontline Nigerian Army personnel. Specifically, the study revealed a significant reduction in PTSD scores following SIT, indicating its potential in mitigating the adverse psychological effects associated with combat exposure. Additionally, the study found no significant differences in posttest PTSD scores based on gender or age, suggesting that SIT is broadly effective across demographic groups within military contexts.These results, therefore, underscore the relevance of SIT as both a preventive and therapeutic tool in military settings, particularly in high-risk operational environments where personnel are repeatedly exposed to combat stressors. The structured nature of SIT, which emphasises cognitive restructuring, relaxation techniques, and problem-solving skills, appears to provide frontline personnel with practical and accessible coping mechanisms to manage stress and maintain operational readiness. Overall, this study contributes to the growing body of evidence supporting psychosocial interventions for trauma-exposed military populations and highlights the need for targeted strategies to enhance psychological resilience among combatants in Nigeria and similar operational contexts. This calls for the integration of relevant psychological interventions in the debriefing schemes of frontline army personnel.
7. Policy Implications and Recommendations
- The findings of this study carry significant implications for military policy, particularly in the Nigerian Army and other similar defense organisations operating in high-risk combat environments. First, the demonstrated effectiveness of Stress Inoculation Training (SIT) in reducing PTSD symptoms suggests that military policymakers should institutionalise SIT as part of pre-deployment, mid-deployment, and post-deployment training programs. This ensures that all personnel, regardless of rank or role, have access to evidence-based psychological resilience training. Second, policymakers should prioritise preventive mental health strategies, incorporating SIT and similar interventions before personnel are deployed to combat zones. Early intervention may help mitigate the development of PTSD and related psychological disorders, reducing long-term treatment costs and maintaining operational readiness. And third, SIT programmes should be embedded within broader mental health policies that include routine psychological assessments, early detection of stress-related symptoms, and continuous monitoring. This ensures a proactive, rather than reactive, approach to mental health management in military contexts.Policy frameworks must allocate adequate resources for training qualified personnel to deliver SIT and provide necessary facilities and materials. Investment in mental health training is critical for sustaining combat effectiveness and the long-term wellbeing of service members.Policies should also extend SIT and related support programmes into post-deployment phases, facilitating smoother reintegration into civilian life and family environments. This may reduce secondary stressors such as social withdrawal, marital conflicts, or occupational challenges.Finally, findings from this and similar studies should inform military mental health policy, emphasising data-driven decision-making to optimize interventions that improve resilience, reduce PTSD prevalence, and enhance operational efficiency.
ACKNOWLEDGEMENTS
- FundingThis research was sponsored by the Tertiary Education Trust Fund (TETFUND) under the approval number REF. NO. TETF/ES/DR&D/CE/NRF2023/HSS/CDS/00015/VOL.I.