-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1118-1122
doi:10.5923/j.ajmms.20261603.56
Received: Jan. 27, 2026; Accepted: Feb. 23, 2026; Published: Mar. 9, 2026

Forensic Criteria for the Evaluation of Sudden Death in Children: Current Approaches and Expert Practice
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKadirov Samat Kuralbaevich
Tashkent Medical University, Tashkent, Uzbekistan
Correspondence to: Kadirov Samat Kuralbaevich, Tashkent Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Sudden death in children presents a significant diagnostic challenge in forensic medicine. This article reviews modern forensic approaches to evaluating sudden death in pediatric populations. We present a classification scheme and a diagnostic algorithm based on autopsy findings, histological examinations, and laboratory analyses. The importance of a multidisciplinary strategy is emphasized, especially in excluding violent causes and understanding underlying pathophysiological mechanisms. Diagnostic complexities, particularly in infants and neonates, are discussed.
Keywords: Sudden death, Children, Forensic pathology, Autopsy, SIDS, Medico-legal evaluation
Cite this paper: Kadirov Samat Kuralbaevich, Forensic Criteria for the Evaluation of Sudden Death in Children: Current Approaches and Expert Practice, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1118-1122. doi: 10.5923/j.ajmms.20261603.56.
1. Introduction
- Sudden death in children remains a critical issue in forensic pathology due to its unpredictable nature and multifactorial causes. Epidemiological data show that a significant number of pediatric deaths remain unexplained even after autopsy [1,2]. The classification and accurate forensic assessment of such cases are crucial for both clinical understanding and legal investigation. This paper aims to consolidate current criteria used in forensic practice and provide a structured approach for the evaluation of sudden pediatric deaths [3,4,5]. Sudden death in children remains one of the most complex and socially significant problems of contemporary forensic medicine, pediatrics, and public health. Despite advances in clinical diagnostics, intensive care, and preventive pediatrics, cases of unexpected and unexplained death in infants and children continue to be reported worldwide, often in the absence of clear clinical precursors. This creates substantial diagnostic, legal, and ethical challenges for forensic experts and healthcare systems [6,7,9]. From a forensic-medical perspective, the evaluation of sudden death in children requires a strictly standardized, evidence-based approach that integrates macroscopic autopsy findings, histopathological examination, toxicological analysis, molecular-genetic testing, and detailed analysis of clinical and circumstantial data. However, in current expert practice, there remains significant variability in diagnostic criteria, interpretation of morphological findings, and attribution of the cause and manner of death. This is particularly relevant in cases of sudden unexplained death in infancy (SUDI), sudden infant death syndrome (SIDS), inherited cardiomyopathies and channelopathies, latent infectious processes, metabolic disorders, and subtle forms of asphyxia [8,10]. The lack of unified forensic criteria often leads to discrepancies between expert conclusions, underdiagnosis of certain pathological conditions, and difficulties in differentiating natural causes of death from external influences or neglect. This, in turn, has direct legal implications, affects the protection of children’s rights, and influences public trust in forensic conclusions. In addition, inaccurate or incomplete determination of the cause of sudden death limits the possibilities for epidemiological analysis, family counseling, and prevention of recurrent fatal outcomes in genetically or environmentally vulnerable groups [11,12]. In recent years, international forensic practice has emphasized the importance of multidisciplinary and multimodal approaches, including immunohistochemical markers of myocardial injury, molecular autopsy, postmortem microbiology, and standardized death scene investigation protocols. Nevertheless, the implementation of these approaches remains uneven, especially in regions with limited access to advanced laboratory technologies. This underscores the need for systematization and critical analysis of current forensic criteria applicable to pediatric sudden death.Therefore, a comprehensive evaluation of modern forensic criteria for the assessment of sudden death in children, with an emphasis on current approaches and expert practice, is highly relevant. Such an analysis contributes to improving diagnostic accuracy, harmonizing forensic methodologies, enhancing expert conclusions, and ultimately supports the development of effective preventive strategies aimed at reducing child mortality from sudden and unexpected causes in the future.The Aim of the Research To study the causes and morphological changes in cases of sudden death in children based on materials from forensic medical examinations conducted at the Republican Scientific and Practical Center of Forensic Medical Expertise during 2021–2025.
2. Materials and Methods
- This study is based on the retrospective analysis of pediatric autopsies conducted at regional forensic centers. Cases classified as sudden and unexplained deaths were selected. Diagnostic procedures included full autopsies, comprehensive histological evaluations, toxicological screenings, microbiological cultures, and, where available, genetic testing. Autopsy protocols were aligned with international guidelines from organizations such as the SIDS and ESPED.
3. Results and Discussion
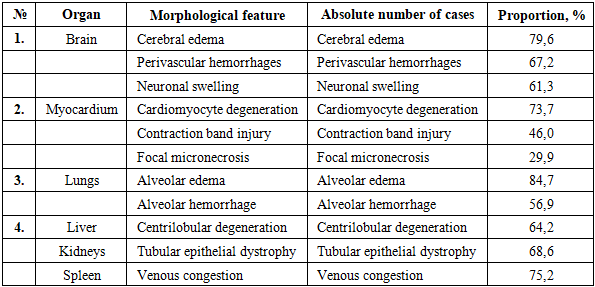
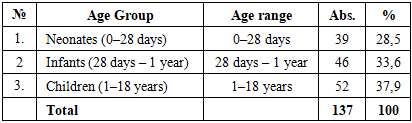
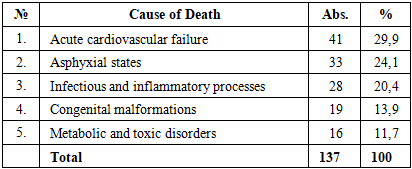
- A total of 137 cases of sudden death in children were analyzed. Morphological examination revealed a consistent complex of terminal and organ-specific changes reflecting hypoxia, shock, and acute circulatory failure. The distribution of pathological findings demonstrated a predominance of generalized hypoxic-ischemic injury affecting the brain, myocardium, lungs, and parenchymal organs.Cerebral pathology was one of the most constant findings. Cerebral edema was detected in 79.6% of cases, representing the dominant morphological sign of acute hypoxia. Perivascular hemorrhages were observed in 67.2%, indicating vascular instability and microcirculatory collapse. Neuronal swelling consistent with acute ischemic injury was present in 61.3% of cases. These findings collectively reflect severe terminal cerebral hypoxia. Myocardial changes were identified in the majority of observations. Cardiomyocyte degeneration was recorded in 73.7%, indicating acute metabolic stress. Contraction band injury, a marker of catecholamine-mediated myocardial damage, occurred in 46.0%. Focal micronecrosis was found in 29.9%, suggesting irreversible myocardial injury in a significant subset of cases. The myocardial findings support the role of acute cardiac dysfunction in the thanatogenesis. Pulmonary pathology was the most frequent organ manifestation of terminal failure. Alveolar edema was detected in 84.7% of cases, representing the highest prevalence among all organs examined. Alveolar hemorrhage was identified in 56.9%, indicating acute respiratory distress and vascular damage. These features confirm severe respiratory insufficiency as a central mechanism in sudden death. The liver demonstrated centrilobular degeneration in 64.2%, reflecting hypoxic injury and circulatory failure. The kidneys showed tubular epithelial dystrophy in 68.6%, consistent with acute shock-related damage. The spleen exhibited venous congestion in 75.2%, indicating systemic circulatory stasis (Table 1). The combination of cerebral edema, myocardial degeneration, pulmonary edema, and parenchymal organ dystrophy forms a reproducible morphological complex corresponding to acute hypoxic-shock syndrome and multi-organ failure. These findings confirm that sudden death in children is most often associated with rapid systemic decompensation rather than isolated organ pathology.
|
|
|
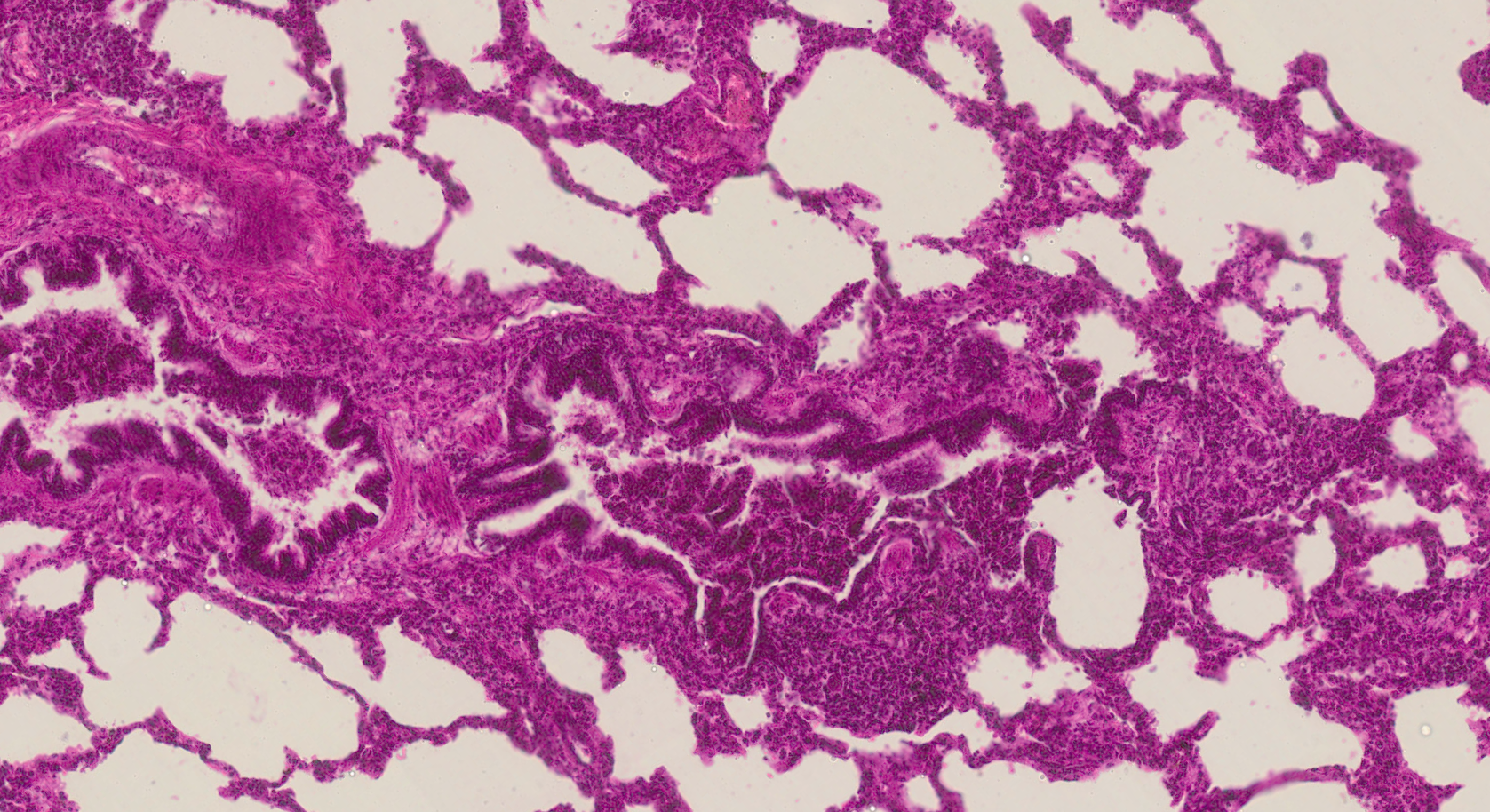 | Figure 1. Lung tissue with marked uneven aeration: a portion of the alveoli is sharply dilated with clear lumina and thinned interalveolar septa, alongside areas of alveolar collapse (atelectasis). The interalveolar septa are locally thickened due to capillary congestion and moderate interstitial edema. The lumina of individual alveoli contain fine eosinophilic proteinaceous material, occasional desquamated alveolocytes, and macrophages. Stained with H&E, mag. 10x20 |
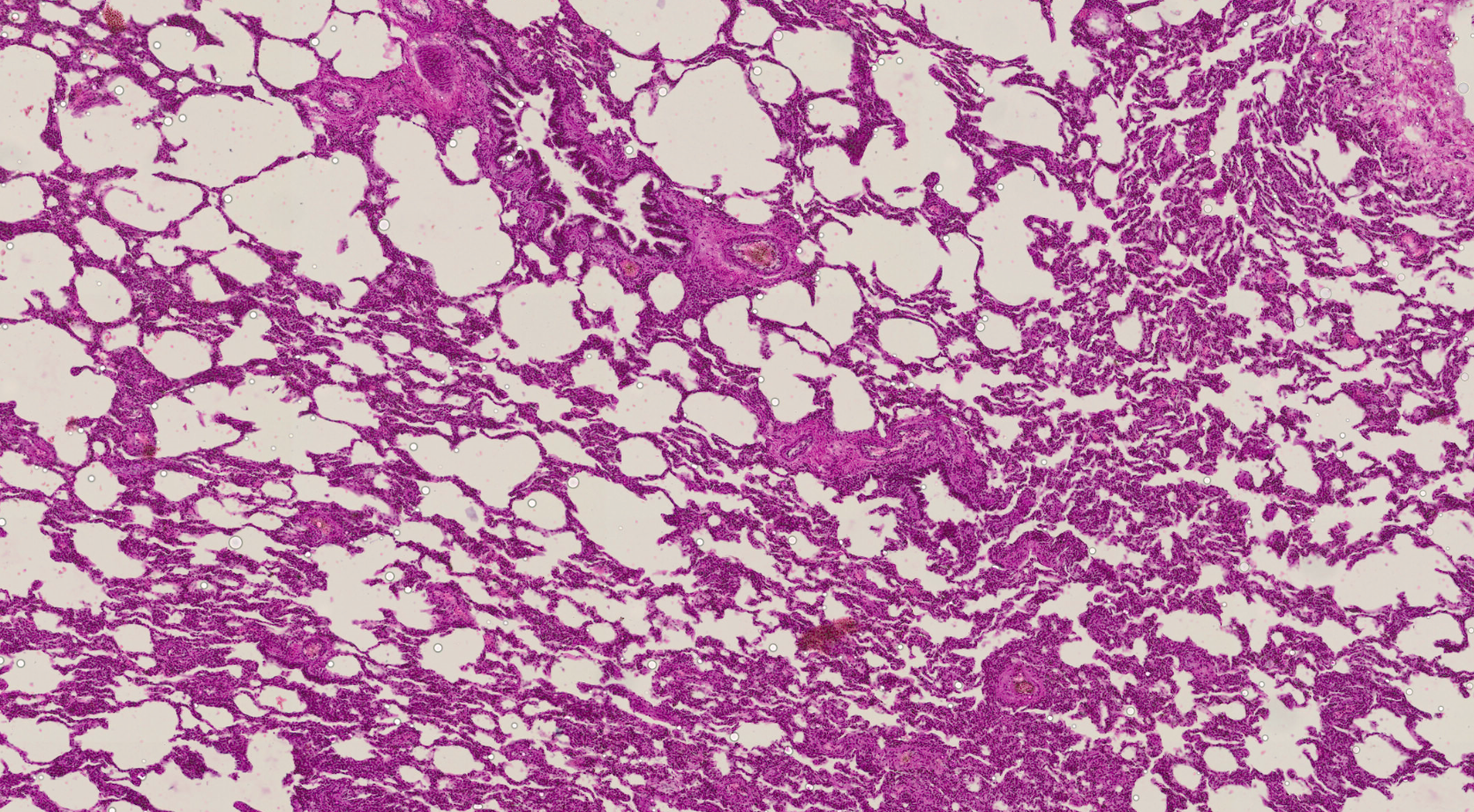 | Figure 2. Lung tissue exhibiting sharply pronounced mosaic ventilation. Alternating areas of severely overdistended, emphysematous alveoli and zones of alveolar collapse (atelectasis) are observed. The interalveolar septa are of uneven thickness, locally thickened due to capillary congestion and interstitial edema. Microcirculatory vessels are dilated, showing signs of venous congestion and stasis. Stained with H&E, mag. 10x20 |
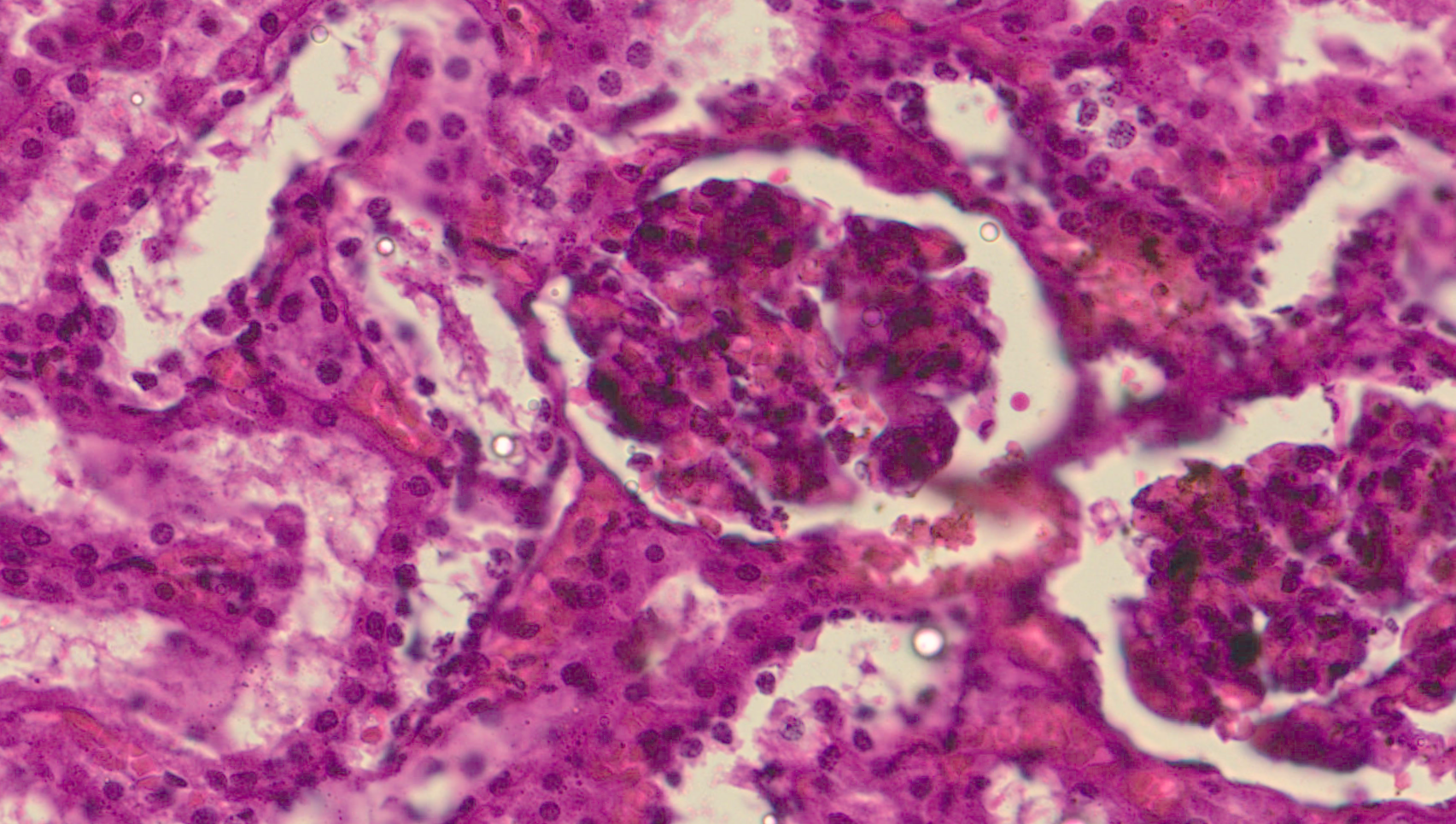 | Figure 3. Kidney tissue specimen. Glomeruli exhibit uneven congestion; capillary loops are dilated, locally showing signs of stasis. Aggregation of formed blood elements is observed in individual glomeruli. The glomerular capsule is moderately dilated, with proteinaceous content present in the lumen. Stained with H&E, mag. 10x20 |
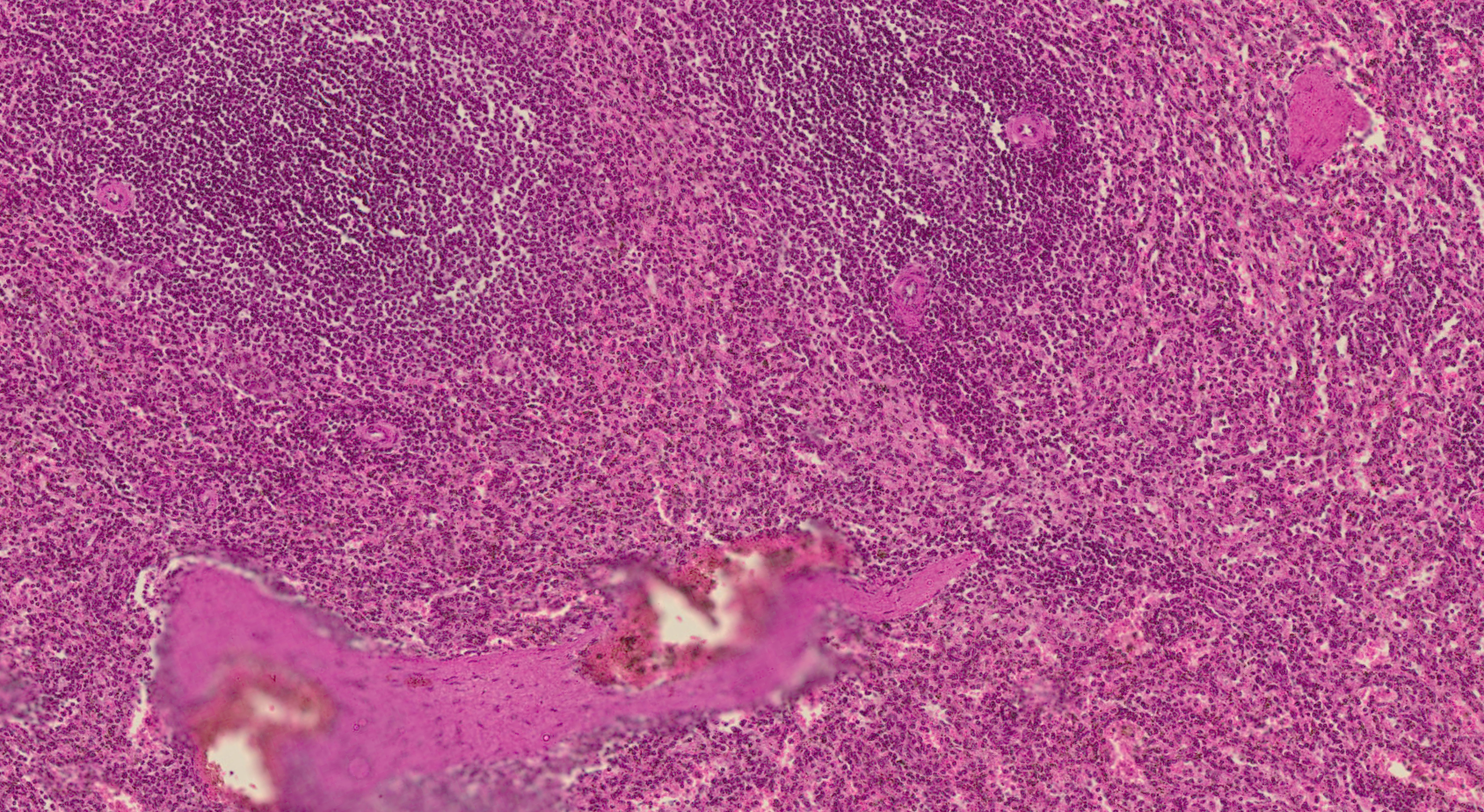 | Figure 4. Spleen tissue specimen. The architecture of the organ is generally preserved. The white pulp is prominent, with enlarged lymphoid follicles showing reactive hyperplasia; the borders between the white and red pulp are locally indistinct. The red pulp is sharply congested; the sinuses are dilated and engorged with formed blood elements. Signs of venous congestion and stasis are observed. Stained with H&E, mag. 10x20 |
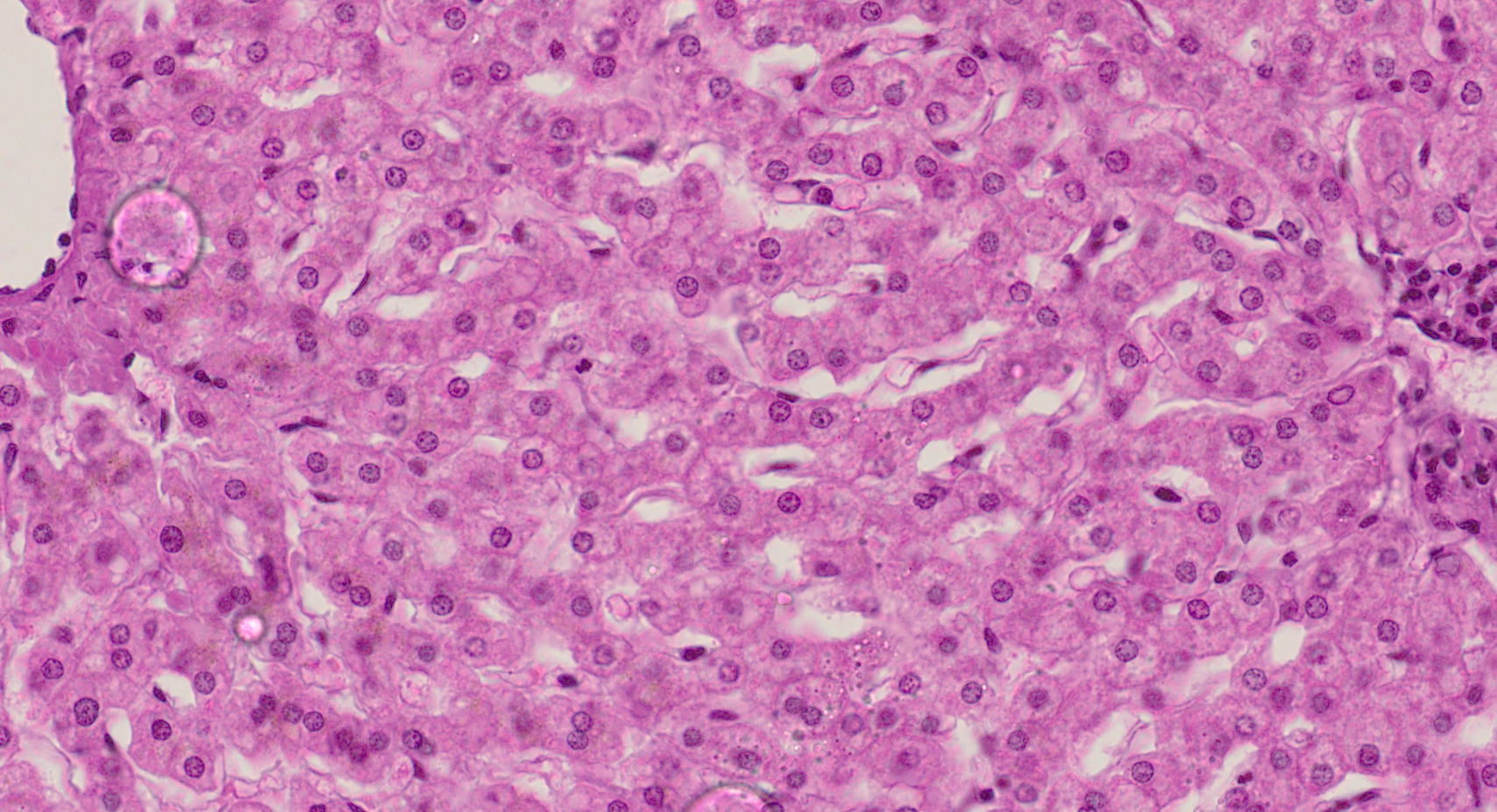 | Figure 5. Liver tissue specimen. The lobular architecture is preserved. Sinusoids are unevenly dilated and congested; localized phenomena of stasis are observed. Hepatocytes exhibit pronounced dystrophic changes: the cells are enlarged, the cytoplasm is granular and vacuolated, and cell boundaries are locally indistinct. Nuclei are predominantly preserved, though some show signs of pyknosis. Stained with H&E, mag. 10x20 |
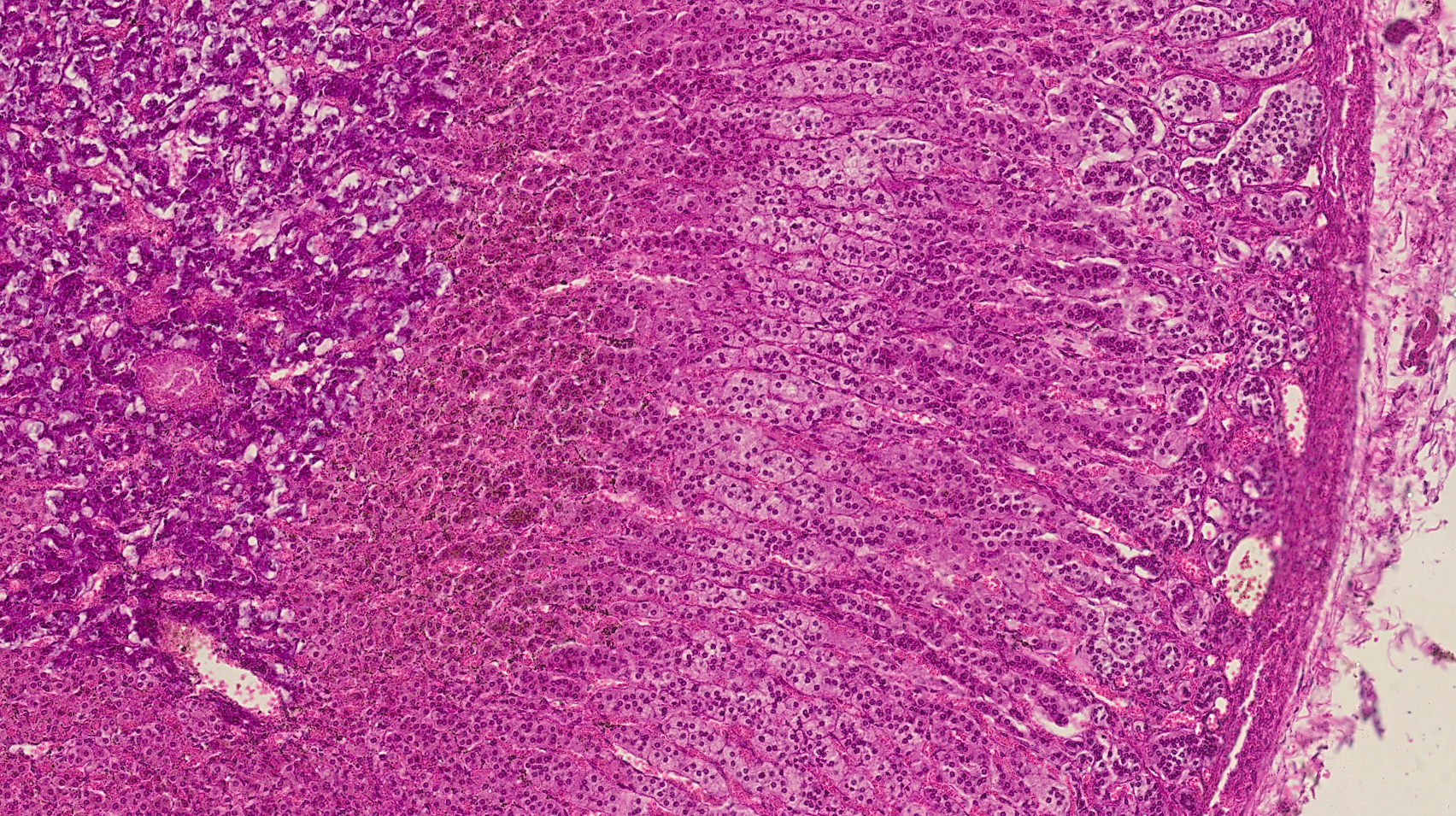 | Figure 6. Adrenal gland tissue specimen. The cortex is preserved, and the zonal architecture is discernible. Cells of the zona fasciculata are enlarged; the cytoplasm is pale and vacuolated, exhibiting signs of fatty and proteinaceous dystrophy. Nuclei are predominantly preserved, though some cells show signs of pyknosis. Sinusoidal capillaries are dilated and congested; phenomena of venous congestion and stasis are observed. The stroma is moderately edematous. Stained with H&E, mag. 10x20 |
4. Conclusions
- The forensic evaluation of sudden death in children must be standardized and comprehensive. Multidisciplinary collaboration is essential, incorporating forensic pathologists, pediatricians, neuropathologists, and geneticists. Enhanced protocols, nationwide databases, and research collaboration are necessary to reduce the number of unexplained pediatric deaths and support preventive strategies. Sudden death in children is accompanied by a typical multi-organ complex of hypoxic-ischemic changes. The most diagnostically significant findings involve the lungs, brain, and myocardium. The early postnatal period represents a high-risk group.The aggregate of identified morphological signs forms objective forensic medical criteria for evaluation. The standardization of histological interpretation enhances the evidentiary value and accuracy of forensic expert conclusions.