Akhmedov I. Yu., Rizaev Zh. A., Yatsyk S. P., Akhmedov Yu. M.
Samarkand State Medical University, Uzbekistan
Correspondence to: Akhmedov I. Yu., Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Obstructive uropathy (OU), particularly hydronephrosis and primary megaureter, represents a leading cause of chronic kidney disease in children. Despite advances in prenatal diagnosis, early identification of predictors—specifically maternal somatic status, obstetric history, and environmental factors—remains insufficiently studied. Objectives: The aim of this study was to analyze the structure of obstructive uropathies and stratify risk factors for their occurrence to optimize perinatal management and prenatal monitoring tactics. Methods: A comprehensive clinical and statistical examination was conducted on 146 pregnant women and their newborns in Samarkand (2020–2026). Participants were divided into a main group (n=61, fetuses/children with verified OU) and a control group (n=85, healthy fetuses). The study utilized antenatal ultrasound with morphometry, Doppler assessment, and postnatal verification. Risk factors were assessed using Odds Ratio (OR) with a 95% Confidence Interval (CI). Results: The study identified significant risk factors for fetal OU. The most critical demographic predictor was late maternal reproductive age (36–40 years), associated with a 9-fold risk increase (OR=9.16). Maternal chronic pyelonephritis (OR=4.35) and iron deficiency anemia (OR=2.59) were leading somatic predictors. Obstetric history analysis revealed that a uterine scar from a cesarean section (OR=3.52) and a history of artificial abortions (OR=2.55) significantly elevated the risk. Environmental factors also played a role; living in rural agricultural areas increased the risk by 2.3 times (OR=2.30), whereas urban living and a healthy lifestyle served as protective factors (OR=0.43). The most severe forms of obstruction manifested early (19–24 weeks, OR=4.34), with peak detection at 30–34 weeks. Conclusions: The development of congenital OU is a multifactorial process driven by a combination of endogenous and exogenous determinants. Pregnant women with identified risk factors (age >35, chronic kidney pathology, compromised obstetric history, and residence in agricultural zones) require inclusion in a high-risk group for targeted prenatal screening to ensure timely diagnosis and treatment.
Keywords:
Congenital obstructive uropathy, Hydronephrosis, Megaureter, Risk factors, Maternal health, Environmental exposure, Epidemiology
Cite this paper: Akhmedov I. Yu., Rizaev Zh. A., Yatsyk S. P., Akhmedov Yu. M., Mapping the Origins of Congenital Urinary Anomalies, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1110-1117. doi: 10.5923/j.ajmms.20261603.55.
1. Introduction
Obstructive uropathy (OU), in particular hydronephrosis and primary megaureter, occupy a leading place in the structure of malformations of the urinary system in children. Despite the improvement of prenatal diagnostic methods, these diseases remain one of the main causes of chronic kidney disease in childhood.The problem of early identification of predictors of the development of this pathology is of particular importance. In modern literature, issues of genetic predisposition and the influence of teratogenic factors are widely discussed, but the role of the somatic status of the mother, obstetric history and social and environmental conditions of the region (in particular, living in rural areas or areas of active farming) has not been studied enough [1,3,6].According to various authors, these anomalies account for up to 20–30% of all developmental defects detected in the prenatal period [9]. They are also the leading cause of end-stage chronic renal failure in children, which determines the high social significance of the problem [8].Antenatally diagnosed hydronephrosis occurs in approximately 1–5% of all pregnancies [12]. Moreover, primary obstructive megaureter is the second most common cause of neonatal hydronephrosis. Its prevalence is estimated to be 1 in 10,000 births [10]. This pathology is characterized by pronounced sexual dimorphism: boys suffer from megaureter 3–4 times more often than girls, while left-sided lesions occur 1.6–4.5 times more often than right-sided lesions [2,7,12].Existing prenatal monitoring algorithms often focus only on the presence of pyelectasis in the fetus, losing sight of a comprehensive assessment of the mother's health. At the same time, identifying high-risk groups based on age, obstetric history and extragenital pathology could contribute to earlier verification of the diagnosis and timely initiation of treatment [13].The purpose of this study was to study the structure of obstructive uropathies and stratify risk factors for their occurrence to optimize perinatal management tactics.
2. Materials and Methods
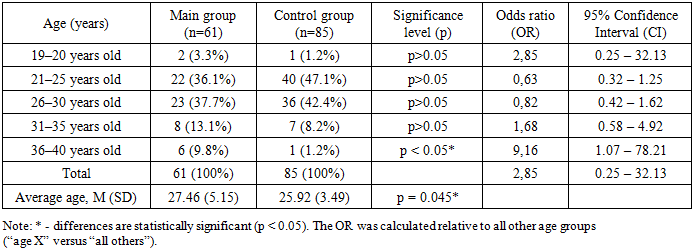
The work is based on the results of a comprehensive clinical and statistical examination and treatment of 146 pregnant women and their newborns who were under observation from 2020 to 2026, at the bases of the Regional Children's Multidisciplinary Medical Center in Samarkand and the multidisciplinary clinic of SamSMU. The study included an assessment of urodynamic parameters in fetuses at the stage of intrauterine development, which made it possible to analyze the formation of physiological mechanisms of urination and identify disturbances in the outflow of urine at the level of the upper and lower urinary tracts during the pathological development of the urinary system. The reliability of the obtained antenatal data was confirmed by the results of subsequent postnatal observation, outpatient and inpatient examinations, as well as surgical treatment of identified malformations.In accordance with the objectives of the study and the antenatal picture identified, all patients were divided into two groups: The main group (n=61) - fetuses and subsequently children with verified obstructive uropathy (hydronephrosis, megaureter, combined defects) and the control group (n=85): fetuses without signs of pathology of the urinary system during the physiological course of pregnancy.The groups were comparable in terms of gestational age at the time of the examination (the average period in the main group was 31.21 ± 3.74 weeks, in the control group - 32.08 ± 3.70 weeks; p > 0.05).Examination methods included collection of somatic and obstetric-gynecological history, assessment of social and household factors and occupational hazards. Instrumental diagnostics in the antenatal period included ultrasound examination with morphometry of the fetal kidneys and Doppler assessment of hemodynamics. Verification of the diagnosis in the postnatal period was carried out using polypositional ultrasound, voiding cystourethrography, excretory urography and dynamic nephroscintigraphy.Statistical data analysis was carried out using the Statistica 10.0 application package.To assess risk factors, the odds ratio (Odds Ratio, OR) with a 95% confidence interval (95% CI) was used. The statistical significance of differences between qualitative characteristics was assessed using the Pearson chi-square test ($\chi^2$). Quantitative parameters are presented as mean and standard deviation (M ± SD), comparisons were made using Student's t test. Differences were considered statistically significant at an error level of p < 0.05.Factors for which the lower limit of the 95% confidence interval exceeded 1.0 were considered clinically significant predictors.The analysis of antenatally diagnosed pathological changes in the urinary system served as the basis for identifying differentiated groups of perinatal monitoring, on the basis of which substantiated approaches to the treatment of children with congenital defects of the urinary system were formulated. The effectiveness of the developed principles is confirmed by positive clinical results in children aged from birth to three years who were treated in the pediatric surgery department of the regional multidisciplinary medical center in Samarkand.Disturbances in the urodynamics of the upper and/or lower urinary tract in the antenatal period were detected mainly in fetuses with pyeloectasia, congenital structural defects of the urinary system, as well as in the presence of combined malformations and pathological course of the intrauterine period.The relevance of maternal age in the occurrence of intrauterine malformations of the fetus, including pathologies of the urinary system, is due to its significant influence on the processes of embryo- and organogenesis. It is known that both young reproductive age of the mother (up to 18 years) and late maternal age (35 years and older) are associated with an increased risk of congenital malformations.Table 1. Characteristics of the age composition of the surveyed groups
 |
| |
|
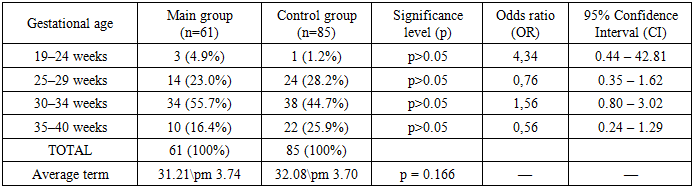
As shown in Table 1, analysis of age characteristics using the calculation of odds ratios (OR) made it possible to stratify the risks of having children with obstructive uropathy depending on the age of the mother. The most favorable age for childbearing in the study population is 21–30 years. For the age intervals of 21–25 years and 26–30 years, the odds ratios were OR = 0.63 and OR = 0.82, respectively (with a 95% CI < 1 at the upper limit for the group of 21–25 years, when compared with the group of 36–40), which characterizes this period as optimal, with a minimal risk of fetal malformation. The key risk factor identified during the study was late reproductive age (36–40 years). For this cohort of women, the odds ratio was OR = 9.16 (95% CI: 1.07–78.21). The lower limit of the confidence interval exceeds one (1.07), which statistically reliably confirms: in mothers over 35 years of age, the risk of having a child with congenital hydronephrosis or megaureter increases by more than 9 times compared to women of other age groups. This fact may be due to the accumulation of genetic mutations in germ cells, a decrease in the body’s reparative capabilities and an increase in somatic burden with age. The results obtained justify the need to classify pregnant women over 35 years of age as a high-risk group for the formation of congenital malformations of the urinary system of the fetus with expanded prenatal screening.To exclude the influence of the gestational factor on the results of morphometry and Doppler measurements, a comparative analysis of the timing of pregnancy (Table 2) at the time of the examination was carried out. It was found that the average gestational age in the main group (n=61) was 31.21\pm 3.74 weeks, in the control group (n=85) - 32.08\pm 3.70 weeks. Statistical analysis did not reveal significant differences between the groups (p = 0.166), which indicates their full representativeness and comparability.Table 2. Distribution of the main and control comparison fetuses according to gestational age
 |
| |
|
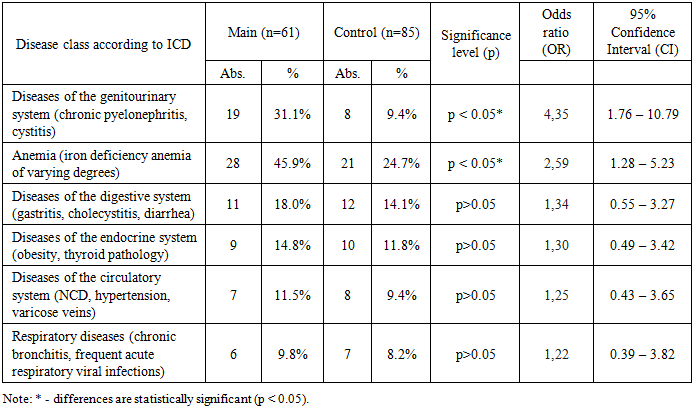
A detailed analysis of the distribution with calculation of the odds ratio (OR) made it possible to identify specific patterns of clinical manifestation of obstructive uropathy depending on the stage of intrauterine development.The period of early manifestation (19–24 weeks), despite the small absolute number of observations, was characterized by the highest odds ratio - OR = 4.34 (95% CI: 0.44–42.81). This indicates that the most severe, clinically significant forms of obstruction, such as megaureter and high-grade hydronephrosis, tend to manifest early and are diagnosed already in the second trimester, requiring timely inclusion of the pregnant woman in the high perinatal risk group.The peak detection of pathology occurred during the period of functional load (30–34 weeks), when 55.7% of patients in the main group were examined. Risk calculation showed an increase in the probability of primary diagnosis of pathology during this period by 1.5 times (OR = 1.56; 95% CI: 0.80–3.02). This fact correlates with the active functional formation of the fetal kidneys, an increase in diuresis and an increase in the hydrodynamic load on the pyelocaliceal system, which leads to the visualization of previously hidden (latent) forms of pyelectasis.By the time of full-term pregnancy (35–40 weeks), there is a natural decrease in the frequency of primary detection of pathology (OR = 0.56), since the main pool of malformations has already been verified by this time. Thus, the absence of statistically significant differences in the average gestational age allows us to assert that the changes in morphometric and hemodynamic parameters identified during the study are due precisely to the presence of an obstructive process, and not to the difference in the age of the fetuses.An important stage of the clinical analysis was the assessment of the somatic health of mothers, since extragenital pathology can act as both a background factor complicating the course of pregnancy and a direct trigger for embryogenesis disorders. To identify predictors of the birth of children with obstructive uropathy, a comparative analysis of the morbidity structure was carried out with the calculation of odds ratios (OR). Data on the incidence of somatic pathology and the magnitude of the risk are presented in Table 3.Table 3. Frequency of occurrence of maternal somatic pathology
 |
| |
|
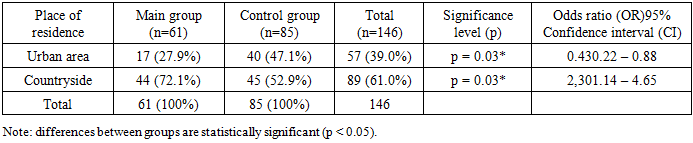
When analyzing the somatic history in Table 3, it was found that patients in the main group had a significantly higher index of somatic burden compared to the control group.In the structure of extragenital pathology, anemia occupied the leading position in both groups. However, in the main group, the incidence of iron deficiency conditions was significantly higher and amounted to 45.9% (28) versus 24.7% (21) in the control group (p < 0.05). Calculation of the odds ratio confirmed the high clinical significance of this factor: OR = 2.59 (95% CI: 1.28–5.23). This indicates that the presence of anemia in the mother increases the risk of obstructive uropathy in the fetus by 2.6 times, which is likely due to the development of chronic hemic hypoxia and impaired tissue metabolism during the period of organogenesis.The most significant specific risk factor was pathology of the mother's urinary system (mainly chronic pyelonephritis in remission). In the main group, this disease was diagnosed in every third pregnant woman - 31.1% (19), which is more than 3 times higher than in the control group (9.4%). For this factor, the maximum odds ratio was obtained: OR = 4.35 (95% CI: 1.76–10.79). Such a high risk (more than a fourfold increase) indicates the presence of a close pathogenetic connection, which may be due to both a genetic predisposition to renal connective tissue dysplasia and the persistence of infectious agents.For other classes of diseases (pathology of the gastrointestinal tract, cardiovascular and endocrine systems), no significant differences were found between the groups (p > 0.05). The odds ratio values for these nosologies were in the range of 1.2–1.3, and the confidence intervals crossed unity, which allows us to exclude them from the leading predictors of the development of congenital hydronephrosis and megaureter in the study population.An important stage in the formation of the medical and social portrait of the women examined was the analysis of their territorial distribution. An assessment of place of residence (urban or rural) was carried out to identify the possible influence of environmental, social and household factors, as well as the availability of qualified prenatal diagnostics on the frequency of detection of congenital malformations of the urinary system.Comparative data on the distribution structure of patients in the main and control groups are presented in Table 4.Table 4. Patient residence structure
 |
| |
|
Analysis of social factors showed an uneven distribution of patients by place of residence. In the overall cohort of those examined, rural residents predominated (61.0%).An intergroup comparison revealed that in the main group the proportion of women living in the village was significantly higher and amounted to 72.1% (44), while in the control group this figure was 52.9% (45) (p = 0.03). Calculation of the odds ratio allowed us to quantify the contribution of this factor: OR = 2.30 (95% CI: 1.14–4.65). This means that living in rural areas increases the risk of having a child with obstructive uropathy by 2.3 times. This fact may indicate the complex influence of unfavorable factors characteristic of rural areas: chemicalization of agriculture (contact with pesticides), drinking habits, as well as lower availability of qualified ultrasound diagnostics in early pregnancy.At the same time, living in an urban area (OR = 0.43; 95% CI: 0.22–0.88) acts as a reliable protective factor, reducing the risk of pathology by more than 2 times. This may be due to better social and living conditions and timely prenatal screening, which makes it possible to identify and correct risk factors at an early stage. The data obtained justify the need to allocate pregnant women from rural areas to a group of increased attention during antenatal monitoring.The study of professional affiliation was carried out in order to identify possible exogenous risk factors, such as physical overexertion or physical inactivity, that could have an indirect effect on embryogenesis.Data on the professional structure with risk assessment are presented in Table 5.Table 5. Patient occupational structure
 |
| |
|
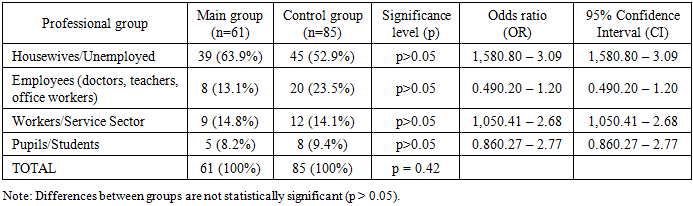
Analysis of socio-professional status showed that the majority of the surveyed population in both groups were housewives and temporarily unemployed women: 63.9% (39) in the main group and 52.9% (45) in the control group. Calculation of the odds ratio showed that belonging to this category slightly increases the likelihood of detecting pathology (OR = 1.58; 95% CI: 0.80–3.09), which is probably associated not with the lack of work as such, but with concomitant physical inactivity and lower social control over the course of pregnancy. Among the working patients of the main group, those employed in the service sector and physical labor (blue-collar professions) predominated - 14.8% (9). The risk for this category (OR = 1.05) is practically equal to one, which indicates the absence of a specific influence of moderate physical labor on the formation of a defect in this sample. The category of employees (mental work) in the main group was 13.1% (8) versus 23.5% (20) in the control. The OR value = 0.49 (95% CI: 0.20–1.20) indicates a tendency towards a protective effect, which may be explained by a higher educational level and discipline in matters of antenatal care, but this trend did not reach statistical significance. Thus, the socio-professional factor is not the leading determinant of the development of obstructive uropathy in the study population.Climatic and geographical characteristics of residential areasConsidering the geographic heterogeneity of the Samarkand region and adjacent areas, to assess the influence of environmental factors on the incidence of congenital kidney defects, an analysis of the distribution of pregnant women by climate zone was conducted, with odds ratios (OR) calculated and presented in Table 6.Table 6. Distribution of patients by climatic and geographical zones
 |
| |
|
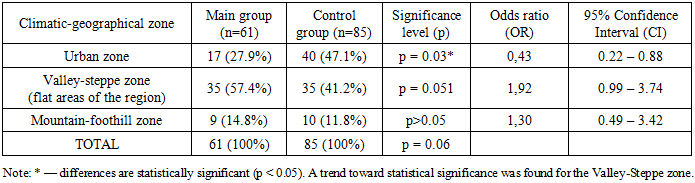
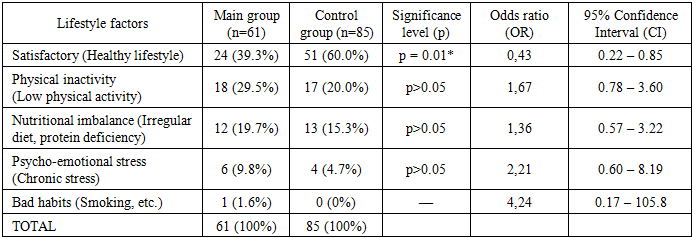
The analysis of the territorial distribution in Table 6 revealed the specifics of the formation of risk groups depending on the zone of residence. The urban zone (Samarkand and others), distinguished by a high population density and accessibility of medical care, was characterized by the lowest risk of pathology. The proportion of urban residents in the main group was 27.9% (17) versus 47.1% (40) in the control. Calculation of the odds ratio showed that living in the city is a reliable protective factor (OR = 0.43; 95% CI: 0.22–0.88), reducing the likelihood of giving birth to a child with a defect by more than 2 times. On the contrary, the valley-steppe zone, which is the main agricultural base of the region with the active use of plant protection products (pesticides, defoliants), was represented by the largest number of patients in the main group - 57.4% (35). In the control group, this figure was 41.2% (35). For this zone, a nearly two-fold increase in risk was established (OR = 1.92; 95% CI: 0.99–3.74). The lower limit of the confidence interval is very close to one, allowing us to interpret the obtained result as a clinically significant trend indicating the probable role of agrochemical pollutants in the teratogenesis of the urinary system. Residents of the mountainous foothill zone constituted 14.8% of the study group and 11.8% of the control group. The OR value of 1.30 (95% CI: 0.49–3.42) indicates the absence of a specific influence of mountain climate factors on the incidence of obstructive uropathies in this sample. Thus, the valley-steppe zone has the most unfavorable risk of congenital kidney defects, which requires increased environmental monitoring and prenatal screening in agricultural areas of the region. The relevance of lifestyle analysis in the development of congenital malformations is due to the direct influence of maternal daily activity and habits on embryogenesis. The study assessed modifiable factors such as diet, physical activity, unhealthy habits, and psychoemotional stress, which can disrupt uteroplacental blood flow and fetal metabolism.An analysis of the lifestyle structure (Table 7) revealed statistically significant differences in the patients' adherence to health-preserving behavior. Only 39.3% (24) of the patients in the study group adhered to healthy lifestyle principles, which is significantly lower than the indicator in the control group - 60.0% (51) (p = 0.01). Calculation of the odds ratio confirmed the high significance of this factor: OR = 0.43 (95% CI: 0.22–0.85). An OR value less than one with statistical reliability indicates that adherence to healthy lifestyle principles is a powerful protective factor, reducing the risk of obstructive uropathies in the fetus by more than 2 times. The low percentage of "healthy" patients in the study group indicates a decrease in the nonspecific resistance of the body of mothers carrying fetuses with urological pathology. Among the unfavorable factors in the main group, physical inactivity was the leading one, diagnosed in 29.5% (18) of women, which is consistent with the high proportion of housewives in this sample and can contribute to venous congestion in the pelvic organs, worsening uteroplacental perfusion. In the control group, this figure was 20.0% (17). Risk assessment showed that physical inactivity increases the likelihood of an adverse outcome by 1.67 times (OR = 1.67; 95% CI: 0.78–3.60), but the confidence interval indicates that this factor is realized mainly in combination with other risks. Alimentary imbalance, characterized by irregular food intake or micronutrient deficiency, was noted in 19.7% (12) of patients in the main group versus 15.3% (13) in the control (OR = 1.36). These differences did not reach statistical significance but indicate a tendency toward nutritional deficiencies in mothers at risk. Psychoemotional stress was twice as common among mothers in the study group as in the control group (9.8% versus 4.7%). Despite the lack of statistical significance according to the chi-square test (p > 0.05), the odds ratio calculation revealed the highest risk value among all modifiable factors: OR = 2.21 (95% CI: 0.60–8.19). This allows us to consider chronic stress as a clinically significant factor that can act both as a cause of embryogenesis disorders (through hormonal mechanisms), and, as a consequence of maternal anxiety about a detected pathology in the fetus. Bad habits (smoking) were isolated (1.6%) and did not have statistical significance in this sample, which is due to the mental characteristics of the population.Table 7. Lifestyle structure
 |
| |
|
To assess the impact of maternal reproductive health on the risk of fetal urinary tract malformations, an in-depth analysis of the obstetric history was conducted. A compromised obstetric history (previous abortions, miscarriages, and uterine surgeries) was considered a marker of potential endometrial and placental dysfunction, which could lead to impaired organogenesis.Data on parity structure and outcomes of previous pregnancies, along with risk assessments, are presented in Table 8.Table 8. Obstetric history structure and pathology risk assessment
 |
| |
|
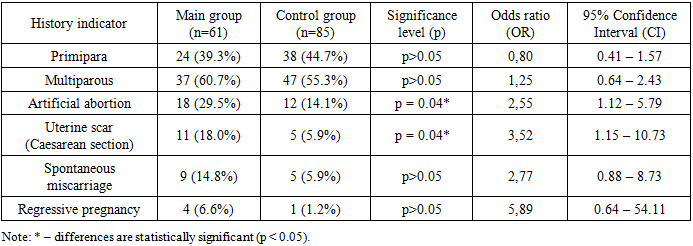
An analysis of the obstetric history revealed that the groups were comparable in terms of parity of births: the proportion of primiparous and multiparous women did not differ statistically (p > 0.05), ruling out the influence of birth order as an independent risk factor in this study.However, when assessing the outcomes of previous pregnancies, a significant association was found between a history of obstructive uropathy and the birth of a child with obstructive uropathy. Thus, a history of artificial abortions was noted in 29.5% (18) of patients in the study group versus 14.1% (12) in the control group. Calculation of the odds ratio confirmed that this factor increases the risk of fetal pathology by 2.5 times (OR = 2.55; 95% CI: 1.12–5.79), which may be associated with endometrial trauma and subsequent placentation disorders. The most significant risk factor was a cesarean section scar on the uterus: the incidence in the study group was 18.0% (11) versus 5.9% (5) in the control group (OR = 3.52; 95% CI: 1.15–10.73).Also noteworthy is a significant trend toward increased risk with a history of spontaneous miscarriages (OR = 2.77) and regressing pregnancies (OR = 5.89). Although these differences did not reach statistical significance (p > 0.05) due to the small absolute number of observations, the high odds ratios (greater than 2.5 and 5, respectively) suggest that recurrent miscarriage is a clinically significant marker of genetic or somatic dysfunction predisposing to malformations in offspring.
3. Conclusions
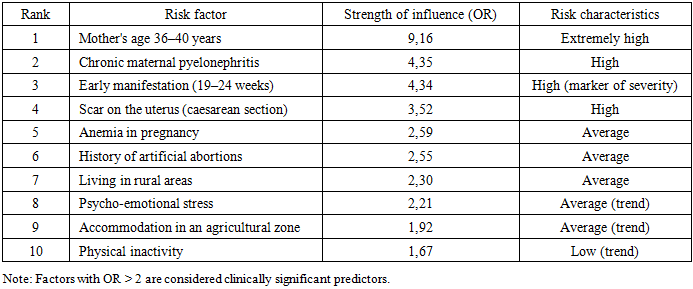
The comprehensive clinical and statistical analysis conducted within Chapter 3 allowed us to develop a medical and social profile of a high-risk patient for the birth of a child with congenital obstructive uropathy. The study results convincingly demonstrate that the development of fetal urinary tract malformations is a multifactorial process in which endogenous (biological) and exogenous (environmental) determinants are closely intertwined. The statistics for these factors are presented in Table 9.Table 9. Distribution of risk factors for the development of obstructive uropathy in the fetus
 |
| |
|
The key demographic predictor of adverse pregnancy outcomes in the study population is late maternal reproductive age. It was found that the age range of 36–40 years is associated with a ninefold increase in the risk of developing pathology (OR=9.16), likely reflecting the accumulation of genetic mutations and a decrease in the body's reparative potential. In contrast, the active reproductive period (21–30 years) is characterized by minimal risk indicators, serving as an optimal time window for childbearing.A close pathogenetic link between the mother's somatic status and the development of the fetal urinary system has been proven. The leading modifiable risk factor is the presence of chronic kidney disease (primarily pyelonephritis) in the pregnant woman, which increases the likelihood of having a child with kidney disease by 4.35 times. This supports the concept of common mechanisms of renal tissue damage in mother and fetus, caused by a genetic predisposition to connective tissue dysplasia or the persistence of infectious agents. An additional significant factor is iron deficiency anemia (OR=2.59), which provokes chronic fetal hypoxia and disrupts organogenesis.Analysis of reproductive history revealed that previous uterine surgeries and artificial abortions are markers of a high probability of developing this defect. The presence of a uterine scar after a cesarean section and a history of abortions increase the risk by 3.5 and 2.5 times, respectively, indicating the role of placental insufficiency and structural and functional endometrial dysfunction in the development of obstructive uropathies.Ecological and geographical factors significantly contribute to the incidence of the disease. Living in rural areas, especially in agricultural valley-steppe zones with active farming, significantly increases the risk of pathology by more than twofold (OR=2.30). At the same time, living in an urban area and maintaining a healthy lifestyle have a significant protective effect, reducing the likelihood of developing the defect (OR = 0.43).A chronological analysis of the detection rate of the pathology showed that the most severe forms of obstruction manifest as early as the second trimester (19-24 weeks), while the peak diagnosis occurs between 30-34 weeks, which coincides with the period of maximum functional load on the fetal kidneys.Thus, based on the calculated odds ratios (OR), a hierarchical risk factor model was constructed to predict the likelihood of having a child with obstructive uropathy and formulate a personalized prenatal care plan.
References
| [1] | McKay A.L., et al. Global epidemiology of congenital anomalies of the kidney and urinary tract (CAKUT): A systematic review and meta-analysis. Journal of Pediatric Urology. 2023; 19(4): 389-400. |
| [2] | Lee R.S., Cendron M., Kinnamon D.D., et al. Antenatal Hydronephrosis as a Predictor of Postnatal Outcome: A Meta-analysis. Pediatrics. 2021; 118(2): 586-593. |
| [3] | Hogan J., et al. Maternal risk factors for congenital anomalies of the kidney and urinary tract: A population-based case-control study. Pediatric Nephrology. 2022; 37(8): 1875-1884. |
| [4] | Tsega T.K., et al. Prevalence and associated factors of congenital anomalies of the kidney and urinary tract among children: A systematic review. Frontiers in Pediatrics. 2024; 12: 1345201. |
| [5] | Nelson C.P., Lee R.S., et al. Ultrasound grading of hydronephrosis: Introduction to the system and reliability analysis. Journal of Pediatric Urology. 2020; 16(3): 321-328. |
| [6] | Benjamin R.H., Stephenson A.J., Sajous M.S. Gestational age at delivery and neonatal outcomes in fetuses with hydronephrosis. Journal of Urology. 2020; 203(4): 789-795. doi: 10.1097/JU.0000000000000615. |
| [7] | Capone V., Gacci A.P., Giannotti M.L. Prenatal diagnosis and management of congenital anomalies of the kidney and urinary tract. Journal of Pediatric Urology. 2021; 17(2): 145-153. doi: 10.1016/j.jpurol.2020.12.005. |
| [8] | Harambat J., van Stralen K.J., Kim J.J., Tizard E.J. Epidemiology of chronic kidney disease in children. Pediatr Nephrol. 2012; 27(3): 363-373. doi: 10.1007/s00467-011-1939-1. |
| [9] | Lauria M., Toenniessen A., Wershba E., Ma Q., Hrab K. Prevalence of Congenital Anomalies of the Kidney and Urinary Tract (CAKUT) in the Greater Buffalo Region: A Retrospective Review. J Urol Ren Dis. 2022; 7: 1284. doi: 10.29011/2575-7903.001284. |
| [10] | Orphanet Report Series, Rare Diseases collection. Prevalence and incidence of rare diseases: Bibliographic data. Orphanet. 2023; 1. Available from: https://www.orpha.net. |
| [11] | Robinson R., Woodward A.J., Whitten M.J. Fetal lower urinary tract obstruction: a review of the literature and proposed multidisciplinary approach to management. Journal of Maternal-Fetal & Neonatal Medicine. 2019; 32(5): 785-792. doi: 10.1080/14767058.2017.1399121. |
| [12] | Sarhan O.M., El Helaly A., Al Otay A., Al Ghanbar M., Nakshabandi Z. Prenatally detected, unilateral, high-grade hydronephrosis: Can we predict the natural history? Can Urol Assoc J. 2018; 12(3-4): E137-E142. doi: 10.5489/cuaj.4587. |
| [13] | Zhang L., Wang Y., Li Y., Liu Y., Zhang Q., Li H., et al. Application of 3D multislice ultrasound in analysis of fetal urinary tract anomalies. Ultrasound in Obstetrics & Gynecology. 2017; 49 (Suppl. 1): 182. doi: 10.1002/uog.18493. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML