-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1105-1109
doi:10.5923/j.ajmms.20261603.54
Received: Jan. 21, 2026; Accepted: Feb. 16, 2026; Published: Mar. 9, 2026

The Significance of the SOD2 Gene Ala16Val Polymorphism in Renal Artery Atherosclerosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNigina Nazarova , Ozimbay Jabbarov
Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Nigina Nazarova , Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

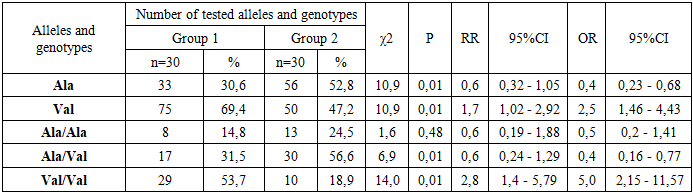
Several scientific hypotheses propose that the Ala16Val polymorphism of the SOD2 gene may influence an individual’s susceptibility or predisposition to renal artery atherosclerosis. Oxidative stress mediated by superoxide radicals, which are regulated by SOD2 (superoxide dismutase 2), is believed to play a critical role in vascular damage and atherogenesis. The present study aimed to examine the potential association between the Ala16Val genetic variant of the SOD2 gene and the occurrence and progression of renal artery atherosclerosis, particularly in patients with chronic heart failure. A total 99 patients: 60 patients with chronic heart failure (NYHA class II) and 39 healthy, age- and sex-matched controls were enrolled in the study. The patient case-control was stratified into two subgroups: first group consist of 30 patients with chronic heart failure without chronic kidney disease (CKD) and second group consist of 30 patients with chronic heart failure with chronic kidney disease. Genotyping was performed using the polymerase chain reaction (PCR) method to identify the presence of the Ala16Val polymorphic variant. The study revealed that the Val allele of the SOD2 gene was significantly associated with chronic kidney disease, suggesting a higher risk in affected patients compared with healthy controls (OR = 1.7, 95% CI: 1.02–2.92, p = 0.01). These findings indicate that the presence of this genetic variant may contribute to the development and progression of renal artery atherosclerosis.
Keywords: SOD2, Renal artery atherosclerosis, Chronic kidney disease
Cite this paper: Nigina Nazarova , Ozimbay Jabbarov , The Significance of the SOD2 Gene Ala16Val Polymorphism in Renal Artery Atherosclerosis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1105-1109. doi: 10.5923/j.ajmms.20261603.54.
1. Introduction
- Renal artery atherosclerosis is a progressive vascular disorder that contributes to the development of chronic kidney disease (CKD) and secondary hypertension, ultimately resulting in increased cardiovascular morbidity and mortality. The pathogenesis of atherosclerosis is multifactorial and involves a complex interaction between genetic predisposition, metabolic abnormalities, and environmental factors [1,2]. Among the key mechanisms driving atherosclerotic vascular damage, oxidative stress plays a central role. Excessive production of reactive oxygen species (ROS) leads to endothelial dysfunction, activation of inflammatory pathways, lipid peroxidation, and structural remodeling of the vascular wall. Antioxidant defense systems, particularly mitochondrial enzymes, are therefore essential for maintaining vascular homeostasis and preventing ROS-mediated injury [4].The superoxide dismutase 2 (SOD2) gene encodes a mitochondrial antioxidant enzyme that catalyzes the conversion of superoxide radicals into hydrogen peroxide and molecular oxygen, thereby protecting cells from oxidative damage. SOD2 is especially important in tissues with high metabolic activity, such as the kidneys and vascular endothelium. A well-characterized functional polymorphism of the SOD2 gene, Ala16Val (rs4880), has been shown to affect mitochondrial targeting efficiency and enzymatic activity. Substitution of alanine (Ala) with valine (Val) in the mitochondrial targeting sequence may impair enzyme transport into mitochondria, resulting in reduced antioxidant capacity [3,5].Carriers of the Val allele are thought to exhibit decreased SOD2 activity, leading to enhanced oxidative stress and increased vulnerability of vascular tissues to damage. This imbalance between ROS generation and antioxidant defense may promote endothelial dysfunction, smooth muscle cell proliferation, and inflammatory responses—processes that are fundamental to the development and progression of atherosclerosis. In the renal circulation, these changes can compromise renal perfusion, accelerate ischemic injury, and contribute to progressive CKD.Although numerous studies have investigated the association between the SOD2 Ala16Val polymorphism and cardiovascular diseases, including coronary artery disease and hypertension, its specific role in renal artery atherosclerosis remains insufficiently explored. Elucidating the contribution of this genetic variant to renal vascular pathology may improve understanding of disease mechanisms, identify individuals at increased risk of CKD progression, and support the development of personalized preventive and therapeutic strategies targeting oxidative stress [6].Several studies have investigated the association between the SOD2 Ala16Val polymorphism and various cardiovascular disorders, including coronary artery disease, peripheral arterial disease, and arterial hypertension. These conditions share common pathogenic mechanisms such as endothelial dysfunction, oxidative stress, inflammation, and vascular remodeling. The SOD2 gene encodes mitochondrial manganese superoxide dismutase, a key antioxidant enzyme responsible for detoxifying superoxide radicals and maintaining redox balance within vascular cells. Functional alterations in this enzyme caused by the Ala16Val polymorphism may lead to impaired mitochondrial antioxidant defense and increased susceptibility to oxidative damage [7].Despite extensive research on the role of the SOD2 Ala16Val variant in cardiovascular pathology, its specific involvement in renal artery atherosclerosis and subsequent chronic kidney disease (CKD) progression remains insufficiently explored. Renal artery atherosclerosis represents a critical vascular condition that compromises renal perfusion, promotes ischemic nephropathy, and accelerates CKD development. Oxidative stress is a central contributor to these processes, driving endothelial injury, smooth muscle cell proliferation, and fibrotic changes in renal vasculature. Therefore, genetic variations that modulate oxidative stress responses, such as the SOD2 Ala16Val polymorphism, may play a decisive role in individual susceptibility to renal vascular injury [8].Investigating the association of the SOD2 Ala16Val polymorphism with renal artery atherosclerosis may provide valuable insights into the genetic predisposition underlying renal vascular diseases. Elucidating the molecular mechanisms linking impaired antioxidant capacity to renal artery damage could improve understanding of CKD pathogenesis and progression. Moreover, identification of high-risk genetic profiles may allow earlier recognition of individuals predisposed to renal artery atherosclerosis and CKD, even before the onset of irreversible structural damage [9,10].Understanding the contribution of the SOD2 Ala16Val variant to renal artery atherosclerosis is essential for the development of preventive strategies and personalized therapeutic approaches. The use of genetic markers associated with increased disease risk may enhance early diagnosis, inform individualized risk stratification, and support targeted interventions aimed at reducing oxidative stress and slowing CKD progression. Ultimately, such an approach has the potential to improve clinical outcomes, reduce cardiovascular and renal complications, and optimize long-term prognosis in patients with renal vascular disease.
2. Material and Methods
- This case–control investigation was carried out at the Tashkent Regional Specialized Somatic Diseases Hospital and involved 60 patients diagnosed with renal artery atherosclerosis and 39 healthy volunteers, all of Uzbek ethnicity and unrelated by lineage. The 60 patients were further categorized into two clinical subgroups: Group 1, comprising 30 patients without chronic kidney disease (CKD), and Group 2, comprising 30 patients with CKD. Inclusion criteria for all participants included abnormal urinalysis findings such as proteinuria and/or hematuria, absence of arterial hypertension prior to disease onset, no history of diabetes mellitus or other systemic comorbidities, no family history of hereditary renal disorders, and at least two generations of Uzbek ancestry.The case-control included 39 healthy individuals with normal urinalysis, normal serum creatinine levels, preserved glomerular filtration rate, and no personal history of kidney disease, hypertension, or diabetes. All participants underwent comprehensive clinical and laboratory assessment, including complete blood count, detailed urinalysis, quantitative 24-hour proteinuria measurement, glomerular filtration rate calculation using the CKD-EPI formula, and 24-hour ambulatory blood pressure monitoring.Genomic DNA was isolated from peripheral venous blood, and the I/D polymorphism of the ACE gene was analyzed using the Rotor-Gene Q programmable thermocycler (QIAGEN) according to the manufacturer’s instructions. PCR amplification was performed with primers flanking the insertion/deletion region in intron 16, and PCR products were resolved via agarose gel electrophoresis to determine Ala/Ala, Ala/Val, and Val/Val genotypes based on fragment size. To ensure accuracy, 10% of samples were randomly re-analyzed, yielding 100% concordance. Negative controls were included in each PCR run, and samples with weak or ambiguous bands were re-tested. Genotype distribution in the control group was assessed for Hardy–Weinberg equilibrium as an additional quality control measure.Statistical analyses included evaluation of allele and genotype frequencies using the chi-square (χ²) test. The relative risk of CKD associated with specific alleles and genotypes was estimated using odds ratios (ORs) and 95% confidence intervals (CIs), calculated with MedCalc software. Further statistical analyses were performed using STATISTICA, and correlations between genetic variants and clinical parameters were assessed using Spearman’s correlation coefficient (r). A p-value < 0.05 was considered statistically significant. All participants provided written informed consent prior to inclusion in the study.
3. Results
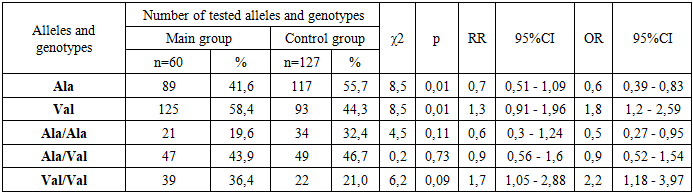
- In the studied main and control groups, the frequency of the ancestral Ala allele was 41.6% and 55.7%, respectively. The frequency of the functional Val allele was 58.4% in the main group and 44.3% in the control group. According to statistical analysis, carriers of the Val allele had a 1.8-fold higher risk of disease development compared to Ala allele carriers, and this difference was statistically significant (χ² = 8.5; p = 0.001; OR = 1.8; 95% CI 1.2–2.59). Conversely, the ancestral Ala allele demonstrated a protective effect against disease development (χ² = 8.5; p = 0.001; OR = 0.6; 95% CI 0.39–0.83).Analysis of the main and control groups revealed that the distribution of Ala/Ala, Ala/Val, and Val/Val genotypes was 19.6%, 43.9%, and 36.4% in the main group, and 32.4%, 46.7%, and 21.0% in the control group, respectively. Statistical evaluation showed that carriers of the Val/Val genotype had a 2.2-fold higher susceptibility to disease development compared to Ala/Val genotype carriers (χ² = 6.2; p = 0.09; OR = 2.2; 95% CI 1.18–3.97). The ancestral Ala/Ala genotype was more frequent in the control group than in the main group (32.4% vs. 19.6%) and was associated with a reduced likelihood of disease development (χ² = 4.5; p = 0.11; OR = 0.5; 95% CI 0.27–0.95). The Ala/Val genotype was slightly less frequent in the main group compared to the control group (43.9% vs. 46.7%) and was not associated with an increased risk of disease (χ² = 0.2; p = 0.73; OR = 0.9; 95% CI 0.52–1.54). The detailed allele and genotype frequencies for the main and control groups are presented in Table 1.
|
|
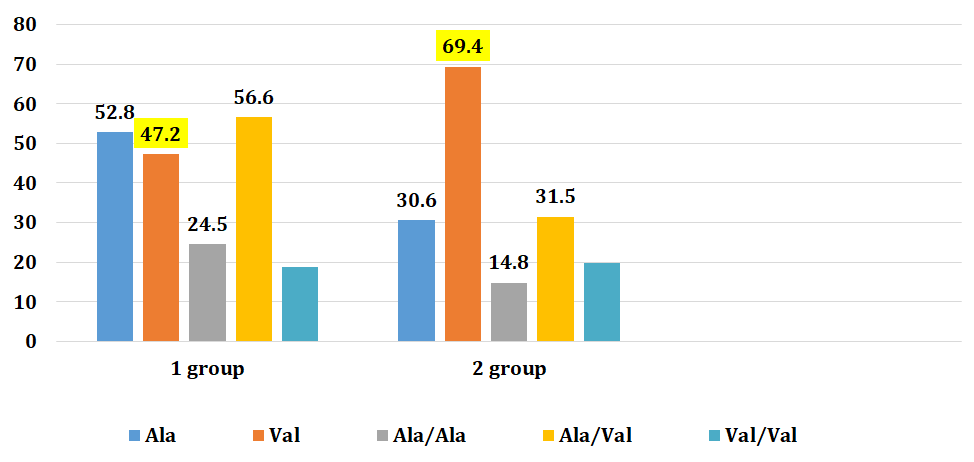 | Figure 1. Comparative distribution of Allele and genotype frequencies of the Ala16Val polymorphism in 1 and 2 groups |
4. Discussion
- The results of this study are consistent with multiple meta-analyses indicating that the SOD2 gene Ala16Val polymorphism exhibits pronounced ethnicity-specific associations with renal diseases. The evidence is particularly robust in Asian populations, where the Val allele and Val/Val genotype have been repeatedly linked to a heightened susceptibility to kidney disorders. For instance, meta-analyses by Tian-biao Zhou et al. (2011) reported a significant positive correlation between the Val allele and chronic kidney disease specifically in Asian cohorts [9], whereas no such association was observed in Arab populations [10].Similar ethnic specificity has been observed for chronic kidney disease (CKD), with Chin Lin et al. (2014) identifying the highest risk among hypertensive Asian males (OR ≈ 3.75), supporting a population-dependent genetic effect [10]. Furthermore, studies on nephrotic syndrome have shown that the Val allele is significantly associated with disease susceptibility in Asian children, while no meaningful correlation has been reported in Caucasian or African populations. These differences may reflect variations in genetic background, environmental exposures, and gene–gene or gene–environment interactions.The biological plausibility of these findings is strengthened by the functional effects of the D allele, which is associated with elevated ACE activity and increased angiotensin II production, leading to enhanced intraglomerular pressure, mesangial proliferation, inflammatory signaling, and fibrosis—key mechanisms in the pathogenesis of glomerular disorders. While current evidence strongly supports an ethnicity-dependent risk pattern, many studies are limited by moderate sample sizes and population heterogeneity, highlighting the need for larger, well-designed, population-specific genetic investigations to clarify the causal contribution of the SOD2 Ala16Val polymorphism to kidney disease susceptibility.
5. Conclusions
- In summary, the results of this study demonstrate a significant association between the Ala16Val polymorphism of the SOD2 gene and the risk of developing chronic kidney disease (CKD) in patients with chronic heart failure. The SOD2 gene encodes manganese superoxide dismutase, an enzyme that plays a critical role in regulating oxidative stress and maintaining mitochondrial function. Dysfunction or altered activity of this enzyme, as influenced by the Ala16Val variant, may contribute to renal vascular injury, progressive kidney damage, and susceptibility to CKD. These findings highlight the importance of genetic factors in the pathogenesis of chronic kidney disease and suggest that the Ala16Val polymorphism could serve as a potential biomarker for early detection and risk stratification in vulnerable patient populations. Furthermore, this study underscores the need for further molecular and clinical investigations to elucidate the precise mechanisms by which SOD2 gene variants influence kidney pathology. Ultimately, understanding the genetic and molecular basis of CKD may provide a foundation for developing novel preventive and therapeutic strategies, enabling more targeted interventions to mitigate disease progression and improve patient outcomes.