-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1102-1104
doi:10.5923/j.ajmms.20261603.53
Received: Feb. 5, 2026; Accepted: Mar. 2, 2026; Published: Mar. 9, 2026

Assessment of the Impact of Obstructive Sleep Apnea Syndrome on Structural and Functional Changes of the Left Ventricular Myocardium in Patients with Arterial Hypertension
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSabirzhanova Zulfiya Talgatovna1, Rakhimova Dilorom Alimovna2
1Tashkent State Medical University, Republic of Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Therapy and Medical Rehabilitation, Republic of Uzbekistan, Tashkent
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Structural and functional changes of the cardiovascular system were determined in patients with arterial hypertension (AH) combined with obstructive sleep apnea syndrome (OSAS). A total of 45 patients with stage I–II AH were examined, including 29 men and 16 women (mean age 60 ± 6.5 years), with disease duration ranging from 5 to 15 years. The presence of obstructive sleep apnea syndrome in patients with AH is associated with more pronounced structural and hemodynamic disorders of the left ventricle (LV) and an increase in left ventricular myocardial mass (LVMM). In patients with AH combined with OSAS, the echocardiographic picture of the heart is characterized by the development of significant cardiac remodeling processes, namely concentric hypertrophy of the left ventricle. Objective of the study: to determine structural and functional changes in the cardiovascular system in patients with arterial hypertension with obstructive sleep apnea syndrome. Material and methods. Forty-five patients with grade I–II arterial hypertension with diagnosed obstructive sleep apnea syndrome were examined to assess the influence of this syndrome on the parameters of the structural and functional state of the myocardium. Results: it was found that the presence of OSAS is reflected in the processes of left ventricular remodeling in arterial hypertension. Comparison of myocardial condition indicators (thickness of the left ventricular walls and their ratio) in patients with and without OSAS showed significant differences. The presence of greater thickness of the interventricular septum (IVS) with relatively equal sizes of the left ventricular cavity indicates the predominance of concentric left ventricular hypertrophy in the presence of OSAS. Conclusion: Obstructive sleep apnea syndrome significantly influences the processes of left ventricular remodeling in patients with arterial hypertension, which dictates the need for early detection of OSAS.
Keywords: Arterial hypertension, Obstructive sleep apnea syndrome, Left ventricular remodeling
Cite this paper: Sabirzhanova Zulfiya Talgatovna, Rakhimova Dilorom Alimovna, Assessment of the Impact of Obstructive Sleep Apnea Syndrome on Structural and Functional Changes of the Left Ventricular Myocardium in Patients with Arterial Hypertension, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1102-1104. doi: 10.5923/j.ajmms.20261603.53.
1. Introduction
- The combination of arterial hypertension and obstructive sleep apnea syndrome is considered in modern medicine as a “vicious circle.” According to classical concepts, each episode of apnea is accompanied by pronounced hypoxemia, hypercapnia, and sharp fluctuations in intrathoracic pressure [3]. These factors cause powerful activation of the sympathoadrenal system, which leads to persistent elevation of arterial blood pressure, especially at night (the “non-dipper” phenomenon), and increases afterload on the left ventricle (LV) [7,10]. A key marker of the negative impact of OSAS in AH is left ventricular hypertrophy (LVH). In patients with combined pathology, LVH occurs significantly more often than in isolated AH [1]. Negative intrathoracic pressure during inspiratory efforts with closed upper airways literally “stretches” the walls of the heart, stimulating mechanical deformation of cardiomyocytes [5]. Hypoxic pulmonary vasoconstriction (Euler–Liljestrand reflex) leads to increased pressure in the pulmonary artery, causing hypertrophy and subsequent dilation of the right ventricle (RV) [9]. The earliest sign of myocardial damage in OSAS is diastolic dysfunction. Impaired myocardial relaxation is associated with the development of interstitial fibrosis and calcium overload under hypoxic conditions [2,6]. In patients with AH, even moderate apnea is associated with a decrease in the ratio of early to atrial filling velocities (E/A) and an increase in isovolumetric relaxation time (IVRT) [8]. Chronic pressure overload and changes in intrathoracic pressure lead to remodeling of the left atrium (LA). An increase in LA volume in OSAS and AH is an independent predictor of atrial fibrillation, which significantly worsens patient prognosis [4,11,12].Aim of the StudyTo determine structural and functional changes of the cardiovascular system in patients with arterial hypertension combined with obstructive sleep apnea syndrome.
2. Materials and Methods
- A total of 45 patients with stage I–II arterial hypertension were examined, including 29 men and 16 women (mean age 60 ± 6.5 years), with disease duration ranging from 5 to 15 years. Verification of the diagnosis was carried out based on the WHO/ISH classification of arterial hypertension (1999). Echocardiography (EchoCG) was performed using a Mindray device (China) in the left lateral decubitus position in M- and B-modes in accordance with the requirements of the American Society of Echocardiography (ASE). The following parameters were assessed: end-diastolic diameter (EDD), end-systolic diameter (ESD), posterior wall thickness of the LV, interventricular septum thickness (IVST), left atrial size (LA), end-systolic volume (ESV), and end-diastolic volume (EDV). LV systolic function was assessed by ejection fraction (EF), calculated using the Teichholz formula [2], and stroke volume (SV), determined as the difference between EDV and ESV. Left ventricular myocardial mass (LVMM) was calculated using the Devereux R.B. formula: LVMM = 1.04 × ((PWT + IVST + EDD)³ − (EDD)³) − 13.6. The LV mass index (LVMI) was calculated as the ratio of LVMM to body surface area. LV hypertrophy was defined as LVMI >125 g/m² in men and >110 g/m² in women. Relative wall thickness (RWT) was calculated using the formula: RWT = (PWT + IVST) / EDD. All patients underwent nocturnal monitoring of arterial blood hemoglobin oxygen saturation (ABHOS) for the diagnosis of OSAS using a portable pulse oximeter “HandHeld Patient Monitor” (China). Depending on confirmation of OSAS, all patients were divided into two groups: Group 1 consisted of 20 patients with stage I–II AH, and Group 2 consisted of 25 patients with stage I–II AH combined with obstructive sleep apnea syndrome. Exclusion criteria were: symptomatic arterial hypertension, history of stroke, myocardial infarction, severe diabetes mellitus, heart failure, presence of cardiovascular diseases that could affect the studied parameters (ischemic heart disease, hemodynamically significant arrhythmias, heart failure, valvular disease, cardiomyopathy, etc.); presence of factors predisposing to sleep apnea syndrome, diseases accompanied by hypertrophy of pharyngeal lymphoid tissue, and endocrine diseases.
3. Results and Discussion
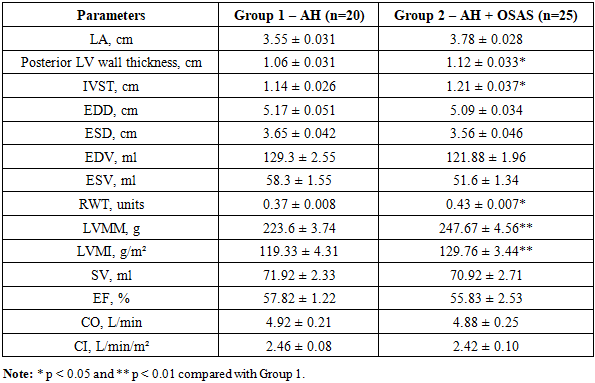
- Assessment of the LV wall condition showed that in the group of patients with AH and OSAS there was a significant increase in IVST, posterior LV wall thickness, RWT, LVMM, and LVMI compared with patients with AH alone. Differences in IVST and posterior wall thickness between Groups 1 and 2 were 5.7% and 6.14%, respectively (p < 0.05). Correspondingly, a statistically significant difference in RWT of 16.2% was also observed between the groups (p < 0.05). The main echocardiographic parameters in examined patients with AH with and without OSAS are presented in Table 1.
|
4. Conclusions
- The presence of obstructive sleep apnea syndrome in patients with arterial hypertension is associated with more pronounced structural and hemodynamic disorders of the left ventricle and an increase in LV myocardial mass. The structural and functional state of the heart in patients with arterial hypertension combined with obstructive sleep apnea syndrome is characterized by more significant remodeling in the form of concentric left ventricular hypertrophy.