M. M. Bakhadirkhanov, N. B. Mirzaeva
Republican Scientific Center for Emergency Medical Care of the Ministry of Health of the Republic of Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The safety and efficacy of early mobilization in patients with ischemic stroke following urgent radiographic endovascular thrombectomy were studied. A total of 140 patients (aged 41–79) were examined and divided into two groups of 70 each: the main group — after urgent radiographic endovascular thrombectomy, and the comparison group — without intervention. Assessments were conducted at baseline, on the 3rd and 7th days based on hemodynamic parameters, heart rate variability, and clinical scales. In the main group, by the 7th day, hemodynamic stabilization was observed against the background of mobilization (reduction in systolic and diastolic blood pressure and heart rate while maintaining SpO₂), as well as recovery of autonomic regulation (decrease in vascular tone index, increase in SDNN, RMSSD, pNN50, elevation of HF, and normalization of the LF/HF ratio). A pronounced improvement in clinical outcomes was also observed in parallel (regression of neurological deficit according to NIHSS, improvement according to mRS, and increase in Barthel index), and by the 7th day, walking recovery reached 82%. Conclusion. Early verticalization after EVT is a safe component of early rehabilitation and is associated with improved autonomic regulation and functional recovery in the first week of the disease.
Keywords:
Ischemic stroke, Endovascular thromboaspiration, Mechanical thrombectomy, Early verticalization
Cite this paper: M. M. Bakhadirkhanov, N. B. Mirzaeva, Justification for Early Verticalization in Patients with Ischemic Stroke After Emergency Radioendovascular Thrombaspiration, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1096-1101. doi: 10.5923/j.ajmms.20261603.52.
1. Relevance
Ischemic stroke (IS) remains one of the leading causes of persistent disability, and the first 7 days of the disease are a critical period that determines the severity of neurological deficits and functional prognosis. In recent years, modern approaches to the treatment of IS have been actively developing, including the expansion of indications for endovascular interventions, as reflected in updated clinical guidelines (in particular, AHA, ASA 2026) [1]. Against the backdrop of widespread adoption of mechanical recanalization for major vessel occlusion (including thromboextraction and thromboaspiration), the importance of optimizing the early recovery phase is increasing, since even with successful reperfusion, the functional outcome largely depends on the timely and safe mobilization of the patient [1,2]. Early verticalization is considered one of the key components of early rehabilitation, potentially accelerating the recovery of motor activity and reducing the severity of life activity limitations. However, excessively early and/or high-intensity mobilization may carry the risk of worsening outcomes, as shown in the large randomized AVERT study, where “very early” and more intensive mobilization within the first 24 hours was associated with a lower likelihood of a favorable functional outcome [3]. This underscores the need for careful selection of timing, intensity, and safety criteria for verticalization, especially in patients after endovascular procedures, when the requirements for hemodynamic stability and cerebral perfusion are particularly high [1]. The use of objective physiological markers to monitor adaptation to vertical load has additional practical significance. One such tool is the analysis of heart rate variability (HRV), which reflects the state of autonomic regulation, the sympathetic-vagal balance, and adaptive reserves. Current reviews and clinical studies show that autonomic dysfunction after stroke is common, can affect prognosis and the rehabilitation process, and HRV parameters (including SDNN and LF/HF) are associated with functional outcomes [4,5].Thus, the development and clinicophysiological justification of approaches to early verticalization in patients with ischemic stroke, especially after endovascular reperfusion, based on hemodynamic and HRV indicators, is a relevant task aimed at increasing the safety of early mobilization and improving functional treatment outcomes [1–5].Research objective: to substantiate the feasibility and safety of early mobilization in patients with ischemic stroke following urgent endovascular thrombectomy, by assessing the dynamics (at baseline, on the 3rd and 7th day) of hemodynamic indicators, heart rate variability parameters, and clinical outcomes, compared to a group of patients who did not undergo urgent endovascular thrombectomy (UET).
2. Materials and Methods of the Research
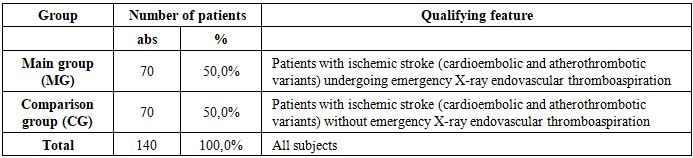
The study was conducted at the neurology department of the Republican Scientific Center for Emergency Medical Care of the Ministry of Health of the Republic of Uzbekistan in 2022–2024. The examination included 140 patients aged 41 to 79 years who were in the hyperacute and acute phases of ischemic stroke (carotid and vertebrobasilar territories). Among them, there were 64 (45.7%) men and 76 (54.3%) women. The diagnosis of ischemic stroke was confirmed based on medical history, neurological examination, and neuroimaging results (CT and/or MRI of the brain).In accordance with the research objective, all patients (n=140) were divided into two equal groups of 70 individuals each: the main group consisted of patients with ischemic stroke (cardioembolic and atherothrombotic variants) who underwent urgent endovascular thrombus aspiration (UETA); the comparison group consisted of patients with ischemic stroke (cardioembolic and atherothrombotic variants) who did not undergo UETA. In the main group (MG), there were 40 (57.1%) women and 30 (42.9%) men; the average age of men was 64.9±8.1 years, and that of women was 68.1±7.5 years. In the comparison group (CG), there were 36 (51.4%) women and 34 (48.6%) men; the average age of men and women was 66.8±8.2 years and 68.0±7.1 years, respectively. (Table 1). Table 1. Characteristics of the Study Groups
 |
| |
|
Patients’ condition was assessed dynamically at three follow-up points: baseline, day 3, and day 7 of observation. Key hemodynamic parameters recorded included systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and oxygen saturation (SpO₂).To analyze autonomic regulation and the adaptive capacity of the cardiovascular system, heart rate variability (HRV) parameters were examined, including the autonomic blood flow index (ABI), temporal HRV parameters (SDNN, RMSSD, pNN50), and spectral parameters (VLF, LF, HF, and the LF/HF ratio). Clinical efficacy was assessed using the NIHSS Neurological Deficit Scale (NIHSS), the mRS Functional Independence Scale (mRS), the Barthel Index, and the proportion of patients who regained walking ability by days 3 and 7.Statistical analysis was performed, with data presented as M±σ. The significance of differences in comparisons between parameters was assessed using the p-value (differences were considered statistically significant at p<0.05).
3. Study Results
Table 2 and Figure 1 show changes in key hemodynamic parameters in patients who underwent RET followed by early verticalization. Analysis of the dynamics revealed a consistent improvement in the adaptive capacity of the cardiovascular system by the seventh day of observation. Table 2. Dynamics of hemodynamic parameters in patients of group II (M±σ)
 |
| |
|
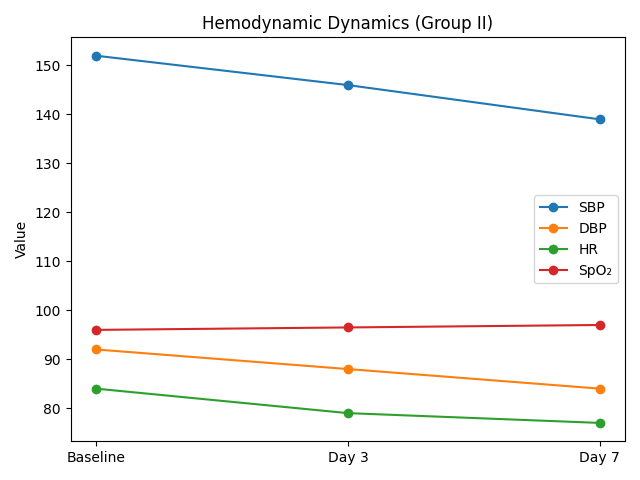 | Figure 1. Dynamics of hemodynamic parameters in patients of Group II (M ± SD) |
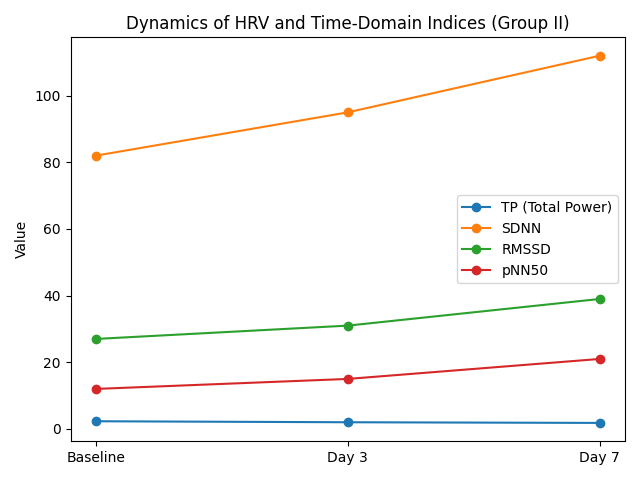
Baseline systolic blood pressure (SBP) in patients was 152.6 ± 12.4 mmHg, corresponding to moderate hypertension. By day 3, a statistically significant decrease to 146.3 ± 11.7 mmHg was observed, and by day 7 it further declined to 138.9 ± 10.5 mmHg. In parallel, diastolic blood pressure (DBP) values also decreased, from 92.7 ± 7.8 mmHg at baseline to 84.2 ± 6.9 mmHg by the end of the week (p < 0.05). This indicates the formation of a more stable and physiologically appropriate level of systemic blood pressure, thereby increasing the safety of verticalization.Heart rate (HR) also demonstrated a favorable trend, decreasing from a baseline value of 84.1 ± 6.5 beats/min to 76.8 ± 6.1 beats/min by day 7. Thus, adaptation of the cardiovascular system to loading occurred through a reduction in sympathetic hyperactivation. SpO₂ values remained stable throughout the entire study period (from 96.2 ± 1.8% to 97.0 ± 1.5%), confirming the absence of any negative effect of early verticalization on gas exchange and tissue oxygenation.Accordingly, the gradual reduction in SBP and DBP indicates that early verticalization contributes to stabilization of arterial blood pressure and reduction of hypertensive load on cerebral vessels. Normalization of HR reflects adaptation of autonomic regulation and attenuation of the stress response to vertical load. Stable SpO₂ values confirm the safety of the method with respect to respiratory function and blood oxygen saturation. Overall, the dynamics of hemodynamic parameters demonstrate that early verticalization is not only safe but also exerts a positive regulatory effect on the cardiovascular system in patients after endovascular reperfusion therapy.Table 3 and Figure 2 present changes in the autonomic circulatory index (ACI) and time-domain HRV parameters in patients after endovascular reperfusion therapy during early verticalization. Positive shifts were already observed by day 3, while by day 7 the changes became statistically significant. At baseline, the mean ACI value was 2.31 ± 0.32, indicating pronounced sympathetic imbalance and low adaptive capacity. By day 3, it decreased to 1.87 ± 0.29, and by day 7 to 1.42 ± 0.25 (p < 0.01).Table 3. Dynamics of FVC and temporary indicators of MIP in patients of Group II (M±σ)
 |
| |
|
 | Figure 2. Dynamics of the VPC and temporal indicators of HRV in patients of group II (M±σ) |
This indicates a normalization of the sympathetic-vagal balance and an increase in the cardiovascular system's resilience to stress. SDNN increased from 82.4±11.6 ms to 112.7±13.5 ms by day 7 (p<0.01), reflecting an overall improvement in heart rate variability and the restoration of autonomic regulation. RMSSD increased from 26.8±4.9 ms to 38.5±6.0 ms (p<0.05), indicating an increase in parasympathetic activity. pNN50 rose from 11.7±3.1% to 20.8±4.1% (p<0.01), confirming activation of vagal influence and enhanced stress resilience of the body.Thus, early verticalization after RET significantly improves the autonomic circulatory index, reflecting the restoration of adaptive reserves. Increases in SDNN, RMSSD, and pNN50 indicate activation of parasympathetic regulation and the development of a more balanced autonomic profile. Positive dynamics of these indices by day 7 underscore the effectiveness of the verticalization technique as a component of early rehabilitation. The combined effects demonstrate that patients in Group II more quickly achieve hemodynamic and autonomic stability, creating conditions for the safe expansion of their physical activity. Table 4 and Figure 3 present changes in the spectral HRV parameters reflecting the distribution of power across different frequency bands in patients after endovascular reperfusion therapy undergoing early verticalization. At baseline, very low frequency (VLF) power accounted for 43.2 ± 6.9%, indicating predominance of humoral–metabolic influences under conditions of pronounced systemic stress. By day 3, this parameter decreased to 39.5 ± 6.1%, and by day 7 to 36.1 ± 5.8% (p < 0.05).Table 4. Dynamics of frequency parameters of HRV in patients of group II (M±σ)
 |
| |
|
 | Figure 3. Dynamics of frequency-domain HRV parameters in patients of Group II (M ± SD) |
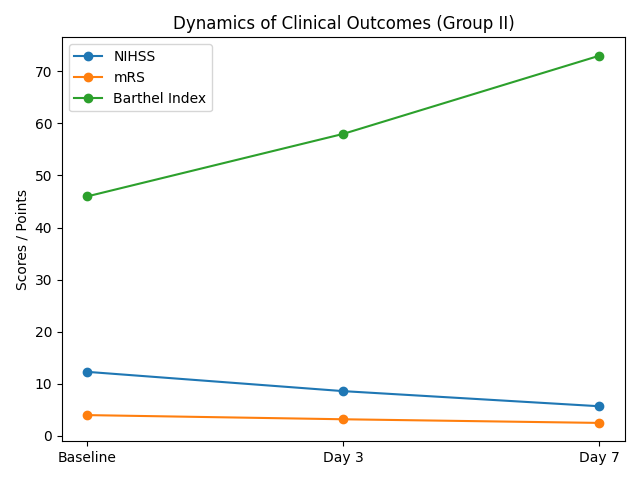
This reflects a gradual decrease in stress-response levels and normalization of metabolic regulation. LF (low-frequency range) was initially 35.1±5.5%, then decreased to 33.8±5.1% on day 3 and 32.2±4.9% on day 7; however, the differences were not statistically significant. This trend indicates a preservation of moderate sympathetic regulation activity, which gradually stabilized. HF (high-frequency range) increased from 21.7±4.3% initially to 26.7±4.6% on day 3 and 31.7±5.2% on day 7 (p<0.01). This statistically significant increase indicates a rise in parasympathetic activity and recovery of relaxation and adaptation mechanisms. The LF/HF index ratio, reflecting the balance of sympathetic and parasympathetic activity, decreased from 1.61±0.32 to 1.02±0.21 by day 7 (p<0.01). Thus, against the background of verticalization, there was an alignment of sympatho-vagal interaction and the formation of an optimal autonomic profile.Thus, a decrease in VLF reflects a reduction in stress response and humoral influence on heart rate. A moderate decrease in LF indicates a reduction in sympathetic hyperactivity, although no statistically significant difference was observed. An increase in HF is an important indicator of enhanced parasympathetic activity and improved adaptive capacity of the body. A decrease in LF/HF to approximately 1.0 confirms the restoration of the sympathovagal balance, which corresponds to physiological norms. The overall changes in spectral parameters demonstrate that the early verticalization method contributes to the harmonization of autonomic regulation and can be considered a safe and effective element of early rehabilitation.Table 5 presents the dynamics of clinical parameters in patients of Group II who underwent early verticalization after endovascular reperfusion therapy. All parameters demonstrated statistically significant improvement during the first 7 days of observation. The baseline NIHSS score (assessment of neurological deficit) was 12.3 ± 3.1 points, corresponding to a moderate stroke severity. By day 3, the score decreased to 8.5 ± 2.6 points, and by day 7 to 5.7 ± 2.2 points (p < 0.01). This indicates a pronounced regression of neurological symptoms and significant clinical improvement associated with early verticalization.Table 5. Dynamics of clinical outcomes in patients of Group II
 |
| |
|
Functional independence assessed by the modified Rankin Scale (mRS) also improved. The baseline mRS score was 4.1 ± 0.6 points, indicating moderately severe disability; by day 3 it decreased to 3.3 ± 0.5, and by day 7 to 2.5 ± 0.4 points (p < 0.01). Thus, most patients transitioned from a state of marked dependence to one of moderate functional limitation.At hospital admission, the Barthel Index (assessment of activities of daily living) was 45.8 ± 6.7 points, reflecting partial dependence. By day 3, the score increased to 58.4 ± 7.1 points, and by day 7 to 72.5 ± 8.3 points (p < 0.01). This indicates restoration of self-care ability and improvement in quality of life. By day 3, independent ambulation was restored in 4% of patients, whereas by day 7 this proportion increased to 82% (p < 0.01), demonstrating that early verticalization substantially accelerated the recovery of motor activity.
4. Conclusions
A statistically significant reduction in the NIHSS confirms the effectiveness of the early standing technique in reducing neurological deficits. Improvements in the mRS and Barthel Index indicate that patients more quickly return to functional independence and self-care. A high rate of walking recovery by day 7 indicates a significant acceleration of the rehabilitation process. The combined positive dynamics of clinical indicators demonstrate that early standing in combination with RET is a safe and effective method for improving outcomes in patients with ischemic stroke.
References
| [1] | Alexandrov A.W., Ansari S.A., Chapman S., et al. 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association // Stroke. 2026. Vol. 57. e•••–e•••. DOI: 10.1161/STR.0000000000000513. |
| [2] | Schellinger P.D., Toni D., de Vries J., White P., et al. European Stroke Organisation (ESO) – European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on Mechanical Thrombectomy in Acute Ischaemic Stroke // European Stroke Journal. 2019. Vol. 4, No. 1. P. 6–12. DOI: 10.1177/2396987319832140. |
| [3] | Bernhardt J., Langhorne P., Lindley R.I., et al.; AVERT Trial Collaboration Group. Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): a randomised controlled trial // The Lancet. 2015. Vol. 386, No. 9988. P. 46–55. DOI: 10.1016/S0140-6736(15)60690-0. |
| [4] | (Authors according to source data). Autonomic dysfunction after stroke: an overview of recent clinical research // Clinical Autonomic Research. 2025. (Publication data according to source: review). |
| [5] | (Authors according to source data). Heart Rate Variability Dynamics as Predictors of Functional Outcome after Acute Ischemic Stroke // Biomedicines (MDPI). 2025. Vol. 13, No. 9. Art. 2217. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML