-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1091-1095
doi:10.5923/j.ajmms.20261603.51
Received: Feb. 3, 2026; Accepted: Feb. 26, 2026; Published: Mar. 7, 2026

Modern Approaches to the Surgical Management of Adnexal Torsion in Girls
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFeruza Abdikarimovna Ibragimova1, Shakhida Dadazhanovna Babazhanova2
1Republican Perinatal Center, Tashkent, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Adnexal torsion represents a critical gynecological emergency in pediatric and adolescent patients, where delayed diagnosis often leads to radical surgery and loss of ovarian function. This study aims to evaluate and compare the efficacy of laparoscopic versus laparotomic approaches in achieving organ-preserving outcomes for adnexal torsion in girls. A retrospective analysis was conducted on 1,175 patients treated between 2019 and 2025, categorized into three groups: newborns with ovarian cysts (n=68), adolescents with confirmed torsion (n=102), and a general pediatric-adolescent cohort (n=1,005). Diagnostic ultrasound with Doppler was employed, and surgical intervention was performed based on strict criteria. Statistical analysis compared outcomes between laparoscopic (n=180) and laparotomic (n=116) procedures. The organ-preservation rate was significantly higher in the laparoscopic group (88.3%) compared to the laparotomy group (61.2%) (χ²=31.6, p<0.001). Ultrasound demonstrated 94.1% sensitivity and 92.3% specificity for diagnosing torsion when cyst size exceeded 50 mm. Laparoscopic detorsion, with or without cystectomy, proved to be the superior surgical strategy, offering a significantly higher likelihood of ovarian salvage, reduced tissue trauma, and shorter recovery. These findings strongly advocate for the standardization of minimally invasive, organ-preserving techniques as the primary management protocol for adnexal torsion in girls to safeguard future fertility and endocrine function.
Keywords: Adnexal torsion, Ovarian cyst, Pediatric gynecology, Organ-preserving surgery, Laparoscopy, Fertility preservation
Cite this paper: Feruza Abdikarimovna Ibragimova, Shakhida Dadazhanovna Babazhanova, Modern Approaches to the Surgical Management of Adnexal Torsion in Girls, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1091-1095. doi: 10.5923/j.ajmms.20261603.51.
Article Outline
1. Introduction
- Adnexal torsion (AT), characterized by the rotation of the ovarian vascular pedicle, is a serious surgical emergency accounting for nearly 3% of all acute gynecological presentations in children and adolescents [1]. The clinical hallmark is often intermittent, nonspecific lower abdominal pain, which contributes to frequent diagnostic delays [2]. Historically, such delays, coupled with the fear of thromboembolism from detorsing an ischemic ovary, led to a high prevalence of radical surgery (oophorectomy) [3]. This approach carries profound long-term consequences, including reduced fertility potential and compromised hormonal development [4].Contemporary evidence has fundamentally altered this paradigm. Studies have conclusively shown that ovarian function can recover after detorsion even in cases of intraoperative cyanosis and apparent necrosis, and the risk of pulmonary embolism is negligible [5,6]. Consequently, the current standard of care emphasizes urgent organ-preserving surgery, with laparoscopic detorsion established as the gold-standard approach [7,8]. This technique maximizes the chance of ovarian salvage while providing the well-documented benefits of minimally invasive surgery.Despite international guidelines, the adoption and success rates of organ-preserving strategies can vary significantly across different clinical settings. This study presents a comprehensive, single-center experience from Uzbekistan, analyzing the diagnostic pathway and surgical outcomes of AT in a large pediatric and adolescent cohort over six years. Our primary objective is to critically evaluate and compare the effectiveness of laparoscopic and laparotomic approaches in achieving ovarian preservation, thereby contributing robust data to support the global shift towards fertility-sparing management of this condition.
2. Materials and Methods
2.1. Study Design and Population
- A retrospective cohort study was conducted at the Gynecological Department of the Tashkent State Medical University Diagnostic Medical Center (TashGMU DMC) from January 2019 to March 2025. The study population was stratified into three distinct groups for detailed analysis:Group I (Neonatal Cysts): 68 female newborns with ovarian cysts diagnosed prenatally or within the neonatal period (0-28 days).Group II (Adolescent Torsion): 102 adolescent females (10-19 years) with a confirmed intraoperative diagnosis of AT.Group III (General Cohort): 1,005 pediatric and adolescent females (0-19 years) hospitalized for the management of ovarian cystic pathology.
2.2. Diagnostic Evaluation
- A standardized protocol was followed for all patients:Documentation of pain onset, character, duration, and associated symptoms (nausea, vomiting, fever). Complete blood count, C-reactive protein, and urinalysis were done in Laboratory Tests: Transabdominal (or transrectal when appropriate) pelvic ultrasonography (US) with pulsed and color Doppler imaging. Cysts were characterized by size, morphology (simple vs. complex), wall features, and vascularity. A size threshold of 40 mm was used to categorize cysts as small (≤40 mm) or large (>40 mm).
2.3. Surgical Indications and Techniques
- Surgical intervention was indicated for: 1) strong clinical/sonographic suspicion of AT, 2) complex cyst morphology, 3) cyst diameter >80 mm, or 4) failure of conservative management. The choice between laparoscopy and laparotomy was based on surgeon judgment, equipment availability, and patient stability.Laparoscopy: A standard three-port technique was used. The torsed adnexa was identified, carefully detorsed, and assessed for viability. Cystectomy or fenestration was performed if a cyst was present. Oophoropexy was reserved for cases with an elongated mesovarium or recurrent torsion.Laparotomy: Performed via a Pfannenstiel or midline incision, adhering to the same principles of detorsion and cyst management. The guiding principle was to preserve the ovary in all cases unless unequivocal, total parenchymal necrosis was observed.
2.4. Statistical Analysis
- Data were analyzed using IBM SPSS Statistics v26.0. Continuous variables are presented as mean ± standard deviation (SD) and compared using the independent samples t-test. Categorical variables are expressed as frequencies (percentages) and analyzed using the Chi-square (χ²) test or Fisher's exact test. Diagnostic test performance (sensitivity, specificity, PPV, NPV) was calculated for ultrasound parameters. A p-value <0.05 was considered statistically significant.
3. Results
3.1. Patient and Clinical Characteristics
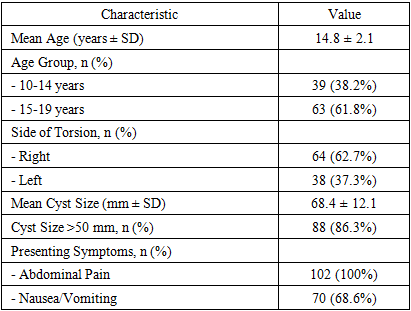
- The total cohort included 1,175 patients. The demographic and clinical profile of the 102 adolescents with confirmed AT (Group II) is summarized in Table 1. The mean age was 14.8 ± 2.1 years. Torsion involved the right ovary in 62.7% of cases. The mean cyst size in torsed adnexa was 68.4 ± 12.1 mm, with 86.3% of cysts measuring >50 mm.
|
3.2. Surgical Outcomes and Approach Comparison
- Of 1,175 patients, 296 (25.2%) underwent surgery. A comparative analysis of surgical approaches is presented in Table 2. Laparoscopy was performed in 180 cases (60.8%) and laparotomy in 116 (39.2%). The organ-preservation rate was significantly higher in the laparoscopic group (159/180, 88.3%) compared to the laparotomy group (71/116, 61.2%) (χ² = 31.6, p < 0.001). Oophorectomy was necessary in 30 cases (10.1% of surgeries), primarily due to extensive necrosis.
|

3.3. Diagnostic Accuracy of Ultrasound
- In patients with surgically confirmed torsion, the combination of a cyst >50 mm and absent Doppler flow had a sensitivity of 94.1%, specificity of 92.3%, PPV of 88.9%, and NPV of 95.7% for diagnosing AT.
3.4. Histopathological Analysis
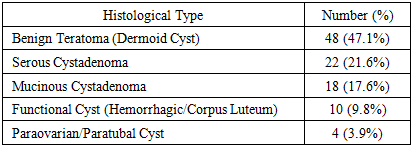
- The histopathological findings for torsed lesions are shown in Table 3. Benign teratomas (dermoid cysts) were the most common pathology (47.1%), followed by serous cystadenoma (21.6%) and mucinous cystadenoma (17.6%).
|
3.5. Neonatal Cohort Outcomes
- In Group I (n=68 newborns), spontaneous regression of cysts occurred in 37 cases (54.4%). Surgery was required in 16 infants (23.5%), with organ-preserving procedures (cystectomy/fenestration) successfully performed in 14 (87.5%).
3.6. Illustrative Clinical Cases
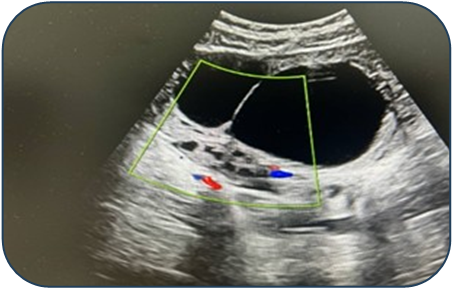
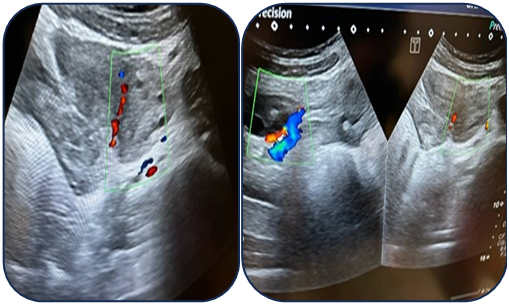
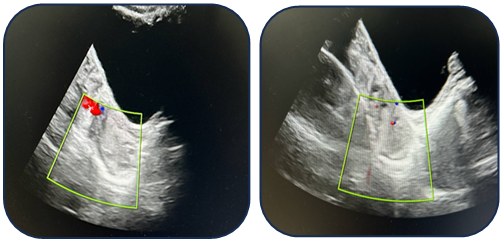
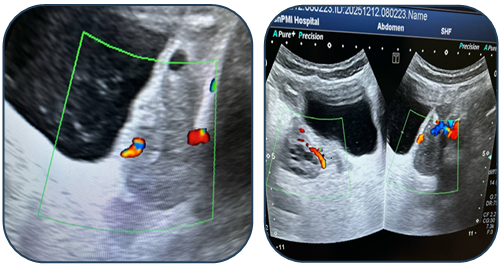
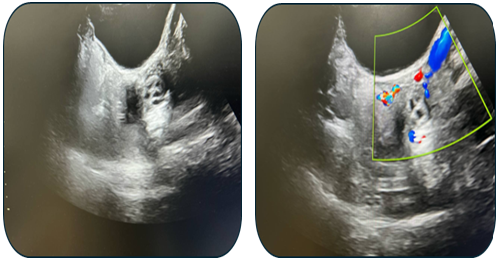
- Case 1: A 17-year-old female presented with acute pain. Ultrasound revealed a 95 mm complex left ovarian cyst with no Doppler flow (Fig. 1). Emergency laparoscopy confirmed a 720-degree torsion. Detorsion and cystectomy were performed. Intraoperative findings are shown in Fig. 2, Fig. 3, and Fig. 4. Histopathology reported a serous cystadenoma. Postoperative ultrasound on day 5 confirmed a viable ovary (Fig. 5).
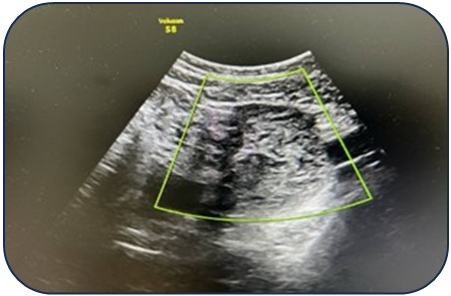 | Figure 1. Ultrasound findings of a left ovarian cyst with torsion |
 | Figure 2. Intraoperative laparoscopic view 1 |
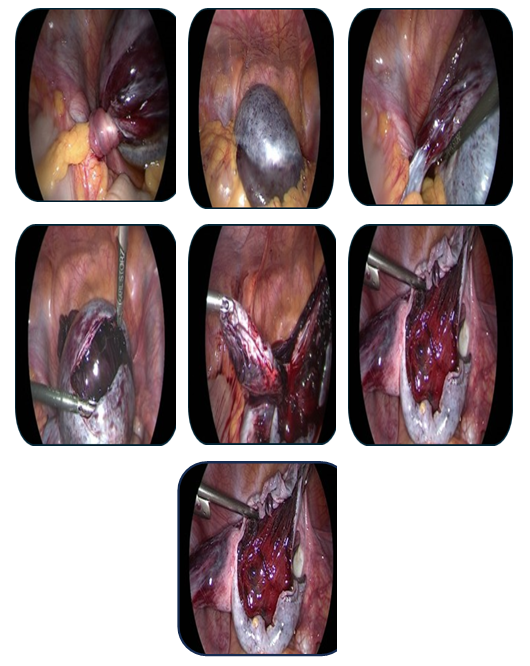 | Figure 3. Intraoperative laparoscopic view 2 |
 | Figure 4. Intraoperative laparoscopic view 3 |
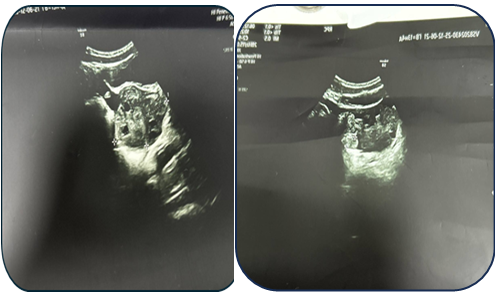 | Figure 5. Postoperative ultrasound examination on day 5 |
 | Figure 6. Preoperative ultrasound examination of the left ovary |
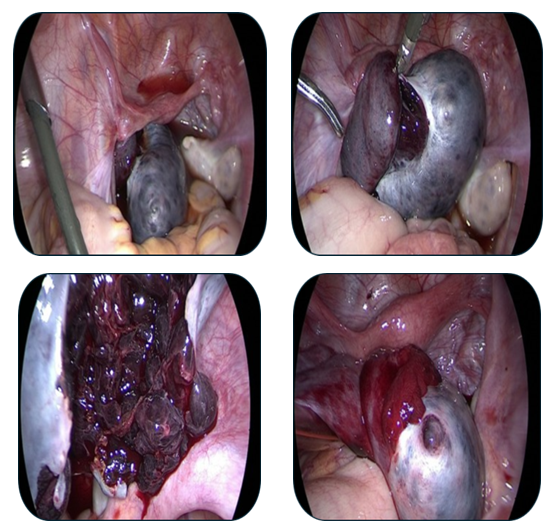
 | Figure 7. Intraoperative laparoscopic view during detorsion 1 |
 | Figure 8. Intraoperative laparoscopic view during detorsion 2 |
 | Figure 9. Ultrasound examination on postoperative day 20 |
4. Discussion
- This large-scale retrospective study provides compelling evidence supporting the central role of laparoscopic organ-preserving surgery in the management of AT in girls. The statistically significant superiority of laparoscopy over laparotomy in achieving ovarian salvage (88.3% vs. 61.2%, p<0.001) aligns with and strengthens existing international literature [7,8]. The lower preservation rate associated with laparotomy may reflect a historical bias towards radical surgery when an ischemic ovary is visualized directly, or a selection bias where more complex cases were initially slated for open surgery.Our findings reaffirm the critical importance of ultrasound with Doppler as the primary diagnostic tool. The high sensitivity (94.1%) and specificity (92.3%) obtained when evaluating cysts >50 mm are consistent with previous reports and highlight a key risk factor [9]. Most importantly, our results and case demonstrations reinforce the fundamental modern principle: the absence of Doppler flow is not a contraindication to detorsion. Ovarian recovery after detorsion, as seen in Case 2, is well-documented and attributed to the organ's dual blood supply [5,6].The histopathological spectrum, dominated by benign neoplasms like teratomas and cystadenomas, underscores the safety of performing conservative cystectomy after detorsion in this population [10]. Furthermore, the high rate of spontaneous resolution in neonatal cysts supports a primarily conservative, observational approach for this specific subgroup [11].The limitations of this study include its retrospective design, potential for selection bias, and the single-center setting, which may affect the generalizability of the findings.
5. Conclusions
- Based on the analysis of 1,175 patients over a six-year period, the following conclusions are drawn:Laparoscopic surgery is the optimal approach for adnexal torsion in girls, yielding a significantly higher rate of ovarian preservation compared to laparotomy.Pelvic ultrasound with Doppler is a highly reliable diagnostic method, with cyst size >50 mm being a major risk indicator.Detorsion should be attempted in virtually all cases, regardless of the ovary's intraoperative appearance, to maximize the potential for functional recovery.A conservative approach is justified for most neonatal ovarian cysts, with surgery reserved for specific complications.Institutional protocols and continued surgical education should be implemented to standardize minimally invasive, organ-preserving techniques as the first-line management for this gynecological emergency.
ACKNOWLEDGEMENTS
- The authors express their sincere gratitude to the medical and nursing staff of the Gynecological Department at the Tashkent State Medical University Diagnostic Medical Center for their dedicated work in patient care and data collection. We also extend our appreciation to the administration of the Republican Perinatal Center and Tashkent State Medical University for their support in facilitating this clinical research.
DISCLOSURE
- The authors declare that there is no conflict of interest regarding the publication of this paper. No financial support or sponsorship was received for this study.