-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 948-950
doi:10.5923/j.ajmms.20261603.21
Received: Feb. 11, 2026; Accepted: Feb. 26, 2026; Published: Mar. 4, 2026

The Impact of Mineral and Acid–Base Metabolic Correction on Postoperative Rehabilitation in Children with Urolithiasis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTukhtaev Firdavs Mukhitdinovich, Kadirov Jonibek Fayzullayevich
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Kadirov Jonibek Fayzullayevich, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Urolithiasis in children is strongly associated with metabolic disturbances that persist even after successful surgical removal of urinary calculi. Disorders of mineral metabolism and acid–base balance play a crucial role in stone recurrence and long-term renal damage. Modern minimally invasive surgical techniques effectively eliminate calculi; however, they do not address the underlying metabolic causes of stone formation. This study analyzes the significance of correcting mineral and acid–base metabolism disorders as a key component of post-operative rehabilitation in pediatric patients with urolithiasis. The findings emphasize that targeted metabolic correction significantly reduces recurrence risk and improves long-term clinical outcomes.
Keywords: Pediatric urolithiasis, Mineral metabolism, Acid–base balance, Metabolic disorders, Postoperative rehabilitation, Stone recurrence, Urinary pH
Cite this paper: Tukhtaev Firdavs Mukhitdinovich, Kadirov Jonibek Fayzullayevich, The Impact of Mineral and Acid–Base Metabolic Correction on Postoperative Rehabilitation in Children with Urolithiasis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 948-950. doi: 10.5923/j.ajmms.20261603.21.
1. Introduction
- Pediatric urolithiasis is increasingly recognized as a chronic metabolic disease rather than an isolated surgical condition [1,2]. Unlike adult stone disease, pediatric urolithiasis is frequently associated with persistent metabolic abnormalities, including hypercalciuria, hypocitraturia, hyperoxaluria, and disturbances in urinary pH regulation [2–4]. These disorders create a favorable environment for crystal nucleation and growth, leading to high recurrence rates after stone removal [3,4].Although minimally invasive surgical techniques—such as ureterorenoscopy, percutaneous nephrolithotomy, and extracorporeal shock wave lithotripsy—have significantly improved immediate treatment outcomes, recurrence prevention remains a major challenge [6,7]. Consequently, postoperative rehabilitation must focus on correcting metabolic and acid–base disorders to achieve sustainable disease control [2,5].
2. Materials and Methods
- Post-operative rehabilitation strategies were analyzed with emphasis on metabolic evaluation and correction. Assessment included biochemical analysis of blood and urine, evaluation of urinary pH, and identification of mineral metabolism abnormalities following surgical intervention [2,4].
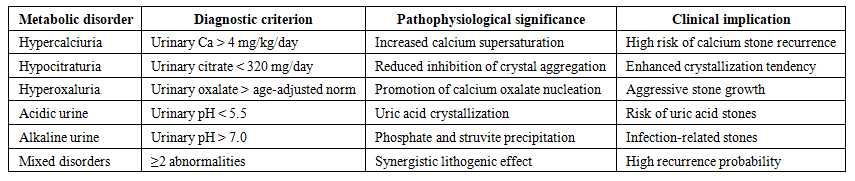 | Table 1. Major Metabolic and Acid–Base Disorders in Pediatric Urolithiasis After Surgical Stone Removal |
3. Results
- Clinical observations indicate that a significant proportion of pediatric patients demonstrate persistent metabolic abnormalities after stone removal. Disorders of calcium metabolism and impaired acid–base balance were among the most prevalent findings [2,4].
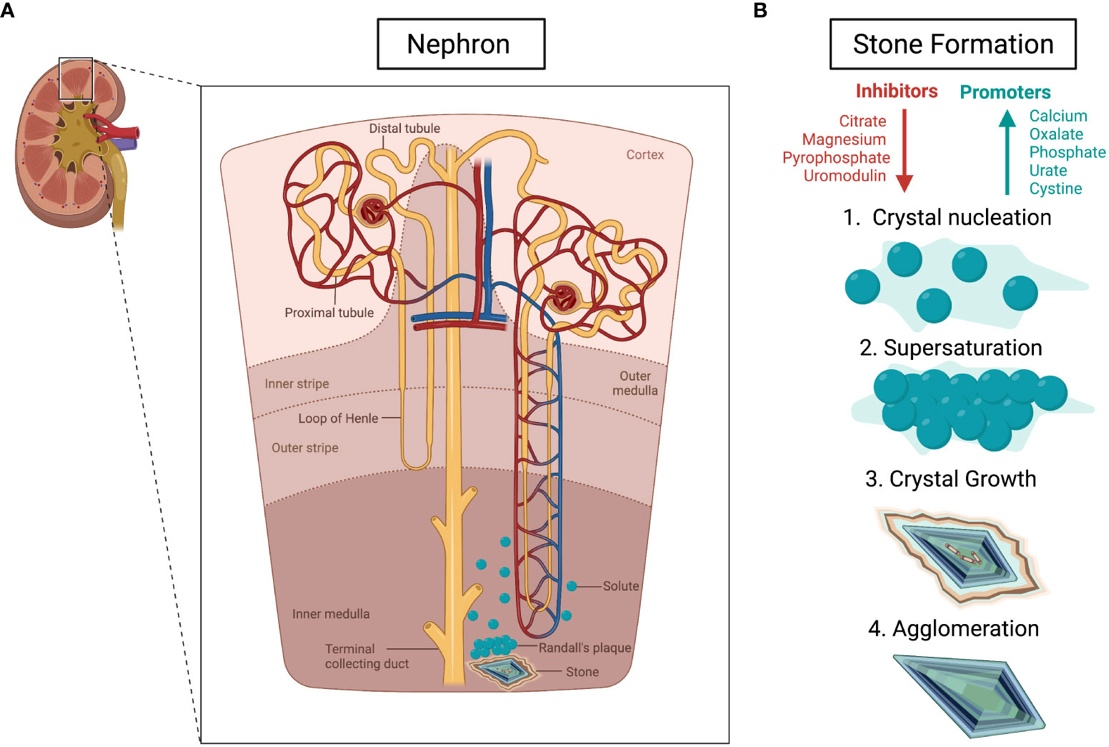 | Figure 1. Pathophysiological mechanisms of nephrolithiasis [5,8]. (A) Formation of renal calculi associated with Randall’s plaque development within the nephron. (B) Sequential stages of kidney stone formation initiated by disruption of the balance between crystallization inhibitors (indicated in red) and promoters (indicated in blue). Arrows denote processes of enhancement (blue) and suppression (red) |
4. Discussion
- Mineral and acid–base metabolism disorders represent fundamental pathogenic mechanisms in pediatric urolithiasis [2,5,8]. Failure to correct these disturbances significantly increases the likelihood of recurrent stone formation, even after technically successful surgery [1,6].Targeted metabolic correction transforms postoperative care from a reactive to a preventive strategy. Individualized rehabilitation programs not only reduce recurrence but also limit the cumulative impact of repeated interventions on renal parenchyma and overall child development.
 | Table 2. Individualized Correction Strategies for Metabolic Disorders in Pediatric Urolithiasis |
5. Conclusions
- Correction of mineral and acid–base metabolism disorders is a cornerstone of effective post-operative rehabilitation in children with urolithiasis. Personalized metabolic management significantly reduces stone recurrence, supports renal function preservation, and improves long-term outcomes [2,5,7]. Post-operative care in pediatric urolithiasis should therefore extend beyond stone removal to include comprehensive metabolic evaluation and targeted correction strategies.