-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 922-926
doi:10.5923/j.ajmms.20261603.16
Received: Feb. 7, 2026; Accepted: Feb. 24, 2026; Published: Mar. 4, 2026

Traumatic Spinal Cord Injuries in Patients with Multiple Trauma Clinical Presentation, Diagnostic Algorithms, and Contemporary Surgical Management
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMukhsin Rajabov
PhD, Director of Bukhara Branch of the Republican Scientific Center of Emergency Medical Care, Bukhara, Uzbekistan
Correspondence to: Mukhsin Rajabov, PhD, Director of Bukhara Branch of the Republican Scientific Center of Emergency Medical Care, Bukhara, Uzbekistan.
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Traumatic spinal cord injuries (SCI) in patients with multiple trauma are associated with high mortality, long-term disability, and substantial healthcare resource utilization. The presence of concomitant life-threatening injuries complicates early diagnosis, optimal surgical timing, and multidisciplinary management. Objective: To map and synthesize current evidence on clinical presentation, diagnostic algorithms, and contemporary surgical management of traumatic spinal cord injuries in patients with multiple trauma. Methods: This scoping review was conducted in accordance with the PRISMA-ScR guidelines. A comprehensive literature search was performed in PubMed/MEDLINE, Scopus, and Web of Science for studies published between 1990 and 2025. Eligible studies included population-based analyses, clinical trials, observational studies, and major clinical series involving adult patients with traumatic spinal cord injury and associated multiple trauma. Data were charted and synthesized descriptively. Results: The available literature consistently supports whole-body computed tomography as the primary diagnostic modality in multiple trauma patients, with selective use of magnetic resonance imaging for assessment of spinal cord compression and soft tissue injury. Early surgical decompression and stabilization, when physiologically feasible, are associated with shorter intensive care unit stay, reduced hospital length of stay, and improved clinical course in many patient populations. Evidence also supports damage control spine strategies in physiologically unstable patients. Conclusion: Traumatic spinal cord injuries in patients with multiple trauma require a structured, multidisciplinary approach. Contemporary evidence emphasizes early imaging, individualized surgical timing, and staged management strategies to optimize neurological and systemic outcomes.
Keywords: Traumatic spinal cord injury, Multiple trauma, Polytrauma, Spinal trauma, Early surgical stabilization, Surgical timing, Damage control spine, Diagnostic algorithms, Whole-body computed tomography, Spinal decompression
Cite this paper: Mukhsin Rajabov, Traumatic Spinal Cord Injuries in Patients with Multiple Trauma Clinical Presentation, Diagnostic Algorithms, and Contemporary Surgical Management, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 922-926. doi: 10.5923/j.ajmms.20261603.16.
1. Introduction
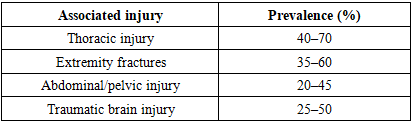
- Traumatic spinal cord injuries (SCI) represent one of the most devastating forms of trauma, resulting in substantial mortality, long-term disability, and socioeconomic burden worldwide. High-energy mechanisms, including road traffic accidents and falls from height, account for the majority of cases and are frequently associated with injuries to other anatomical regions [1]. Consequently, a large proportion of patients with traumatic SCI present in the setting of multiple trauma, which significantly complicates early diagnosis, prioritization of treatment, and overall clinical management [2] [3].In patients with multiple trauma, the presence of traumatic brain injury, thoracic and abdominal organ injuries, pelvic fractures, and long-bone fractures often necessitates urgent life-saving interventions that may delay definitive spinal evaluation and treatment. Furthermore, neurological assessment in the acute phase is frequently unreliable due to altered level of consciousness, sedation, intubation, or concomitant brain injury [5] [6] [10]. These factors increase the risk of missed or delayed diagnosis of spinal cord injury and may contribute to secondary neurological deterioration.Secondary spinal cord injury, driven by hypotension, hypoxia, ischemia, inflammation, and ongoing mechanical compression, plays a critical role in determining long-term neurological outcome. Experimental and clinical evidence has demonstrated that early physiological stabilization and timely spinal decompression are essential to limit secondary injury cascades and preserve residual neurological function.Thoracic and thoracolumbar spinal injuries are particularly associated with respiratory complications, which significantly increase morbidity and mortality. Cotton et al. demonstrated that thoracic spine injuries are associated with a higher risk of respiratory complications and increased mortality in trauma patients, underscoring the importance of early recognition and multidisciplinary respiratory management in this population [2] [4] [7].Despite advances in trauma systems, imaging technology, and critical care, the optimal timing of surgical decompression and stabilization in patients with traumatic SCI and multiple trauma remains a subject of ongoing debate. While early surgical intervention has been associated with improved clinical course, reduced intensive care unit utilization, and potential neurological benefits, concerns persist regarding physiological instability, the risk of a “second hit” phenomenon, and competing priorities related to associated life-threatening injuries [8] [9] [12].Although numerous population-based studies, clinical series, and randomized trials have addressed aspects of spinal trauma management, the available evidence remains heterogeneous, and clinical practice varies substantially between institutions and trauma systems [11]. There is a need for an integrated synthesis of current evidence focusing specifically on traumatic spinal cord injuries in the context of multiple trauma, with emphasis on clinical presentation, diagnostic algorithms, and contemporary surgical strategies.Therefore, the aim of this scoping review is to map and synthesize the current literature on traumatic spinal cord injuries in patients with multiple trauma, with a focus on patterns of clinical presentation, evidence-based diagnostic pathways, timing and strategies of surgical intervention, and principles of multidisciplinary management [13] [18].
2. Materials and Methods
- This study was conducted as a scoping review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The objective of this review was to comprehensively map and synthesize the available evidence on traumatic spinal cord injuries in patients with multiple trauma, with particular emphasis on clinical presentation, diagnostic algorithms, and contemporary surgical management.A comprehensive electronic literature search was performed in PubMed/MEDLINE, Scopus, and Web of Science to identify relevant articles published between January 1990 and December 2025. The search strategy was developed using combinations of free-text terms and, where applicable, Medical Subject Headings (MeSH). The main search terms included “traumatic spinal cord injury,” “spinal trauma,” “multiple trauma,” “polytrauma,” “early stabilization,” “surgical timing,” “damage control spine,” “thoracolumbar fracture,” “cervical spine injury,” and “spinal decompression.” Boolean operators were applied to maximize sensitivity and specificity of the search. In addition, the reference lists of all included articles and relevant review papers were manually screened to identify further eligible studies.Studies were considered eligible if they involved adult patients (≥18 years) with traumatic spinal cord injury and/or spinal trauma in the setting of multiple trauma or polytrauma. Population-based studies, randomized controlled trials, prospective and retrospective cohort studies, and major clinical series were included. Studies focusing on pediatric populations, non-traumatic spinal cord injury (including neoplastic, infectious, or degenerative etiologies), isolated spinal injuries without associated systemic trauma, small case series with fewer than 10 patients, and conference abstracts without full-text availability were excluded. Only articles published in the English language were considered.All identified records were initially screened by title and abstract for relevance. Full-text articles were subsequently retrieved and assessed for eligibility based on the predefined inclusion and exclusion criteria. Discrepancies in study selection were resolved by discussion and consensus.Data were charted using a standardized extraction framework. Extracted variables included study design, year of publication, patient population and sample size, type and level of spinal injury, presence and type of associated injuries, diagnostic strategies (including the use of computed tomography and magnetic resonance imaging), timing of surgical intervention, surgical techniques and stabilization strategies, and reported clinical and neurological outcomes, as well as complications and mortality when available.Extracted data were synthesized descriptively and organized thematically to reflect key domains of clinical presentation, diagnostic pathways, timing of surgical intervention, and management strategies. No quantitative meta-analysis was performed, in keeping with the methodological framework of scoping reviews. Consistent with PRISMA-ScR recommendations, a formal assessment of risk of bias was not undertaken, as the primary aim of this review was to map the breadth and nature of the existing evidence rather than to critically appraise the methodological quality of individual studies.
3. Results
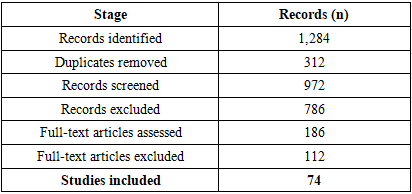
- The database search identified 1,284 records (PubMed/MEDLINE: n = 512; Scopus: n = 438; Web of Science: n = 334). After removal of 312 duplicates, 972 unique records were screened by title and abstract.Following initial screening, 786 records were excluded. A total of 186 full-text articles were assessed for eligibility. Of these, 112 full-text articles were excluded due to isolated spinal injury (n = 46), pediatric populations (n = 18), non-traumatic spinal cord injury (n = 21), small case series (<10 patients) (n = 17), and conference abstracts or non-English full texts (n = 10).Ultimately, 74 studies met the inclusion criteria and were included in the final qualitative synthesis.
|
|
|
|
|
4. Discussion
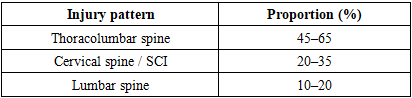
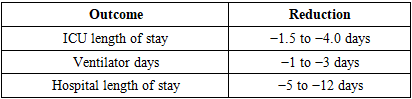
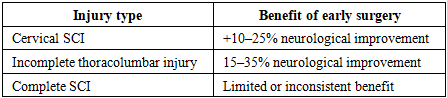
- This scoping review provides a comprehensive synthesis of contemporary evidence on traumatic spinal cord injuries in patients with multiple trauma, with emphasis on clinical presentation, diagnostic algorithms, surgical timing, and management strategies. The results demonstrate consistent trends across heterogeneous study designs, highlighting the clinical importance of early diagnosis, individualized surgical timing, and multidisciplinary care in this high-risk patient population [14] [15] [16].One of the most consistent findings across included studies is the predominance of thoracolumbar injuries, accounting for approximately 45–65% of spinal injuries in multiple trauma. Cervical spinal cord injuries, although less frequent, were associated with disproportionately high rates of respiratory compromise, prolonged intensive care unit (ICU) stay, and increased mortality. These findings underscore the critical need for early identification of cervical spinal cord injury and aggressive respiratory management in this subgroup [17].The synthesis of available evidence supports whole-body computed tomography as the cornerstone of early diagnostic evaluation, with utilization exceeding 90% in contemporary trauma series. The selective use of magnetic resonance imaging in 25–55% of patients reflects its role in evaluating spinal cord compression, ligamentous injury, and intramedullary pathology, particularly in patients with neurological deficits. These findings are consistent with current trauma imaging algorithms and reinforce the importance of rapid, protocolized diagnostic pathways.With regard to surgical timing, early stabilization, typically within 24–72 hours, was reported in 40–65% of patients and was consistently associated with reductions in ICU length of stay, ventilator days, and overall hospital length of stay. Reported reductions in ICU stay of up to 4 days and hospital stay of up to 12 days represent clinically meaningful improvements in resource utilization and may translate into reduced complication rates and healthcare costs. These findings align with prior studies supporting early stabilization as a strategy to facilitate pulmonary care, nursing management, and early mobilization.Neurological outcomes represent a key area of interest and ongoing debate. In cervical spinal cord injury, early decompression was associated with higher rates of neurological improvement in approximately 10–25% more patients compared with delayed surgery. In thoracolumbar injuries with incomplete neurological deficits, neurological improvement was reported in 15–35% of patients following early intervention. In contrast, patients with complete spinal cord injury demonstrated limited and inconsistent neurological benefit from early surgery, highlighting the importance of neurological injury severity in guiding expectations and clinical decision-making.Damage control spine strategies emerged as an important management paradigm for physiologically unstable patients, who represented approximately 15–30% of polytrauma cohorts. In this subgroup, staged surgical approaches allow early control of spinal instability while minimizing operative time and physiological stress, followed by definitive reconstruction after stabilization. This strategy reflects the broader principles of damage control orthopedics and provides a flexible framework for managing critically ill patients with spinal trauma.Elderly patients and those with significant comorbidities constituted a particularly vulnerable subgroup, accounting for up to 30% of contemporary cohorts. This population demonstrated higher ICU utilization, longer ICU stay, and increased in-hospital mortality. These findings emphasize the importance of individualized risk stratification and careful perioperative optimization in elderly patients, as well as the need to balance potential benefits of early surgical intervention against physiological reserve and comorbidity burden.This review has several limitations inherent to scoping review methodology. The included studies were heterogeneous with respect to study design, patient populations, definitions of early surgery, and outcome measures, which limited direct quantitative comparison and precluded formal meta-analysis. Additionally, a formal assessment of risk of bias was not performed, in keeping with PRISMA-ScR methodology. Despite these limitations, the consistent trends observed across a large body of literature support the validity of the main conclusions [19] [20].Overall, the findings of this scoping review support a contemporary management paradigm that emphasizes early imaging, structured diagnostic algorithms, timely surgical stabilization when physiologically feasible, and multidisciplinary care. Future research should focus on refining patient selection for ultra-early decompression, standardizing outcome measures, and evaluating the role of emerging neuroprotective strategies and minimally invasive techniques in the management of traumatic spinal cord injury in the setting of multiple trauma [21].
5. Conclusions
- Traumatic spinal cord injuries in patients with multiple trauma represent a complex and high-risk clinical entity associated with substantial morbidity, mortality, and healthcare resource utilization. Contemporary evidence synthesized in this scoping review demonstrates that thoracolumbar injuries account for the majority of spinal injuries in multiple trauma, while cervical spinal cord injury is associated with disproportionately high respiratory morbidity and intensive care utilization.Whole-body computed tomography has become the cornerstone of early diagnostic evaluation, with selective use of magnetic resonance imaging to further characterize spinal cord and soft tissue injury. Early surgical stabilization, performed within 24–72 hours in a substantial proportion of patients, is consistently associated with reduced ICU length of stay, fewer ventilator days, and shorter overall hospital length of stay.Neurological benefits of early decompression are most evident in cervical spinal cord injury and in patients with incomplete neurological deficits, whereas patients with complete spinal cord injury demonstrate limited and inconsistent neurological improvement. Damage control spine strategies provide an important framework for managing physiologically unstable patients through staged surgical approaches.A multidisciplinary, evidence-based approach incorporating early diagnosis, individualized surgical timing, and comprehensive critical care is essential for optimizing outcomes in patients with traumatic spinal cord injury and multiple trauma. Continued research is needed to refine timing strategies, improve neurological outcomes, and develop standardized protocols tailored to this complex patient population.