-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 913-915
doi:10.5923/j.ajmms.20261603.14
Received: Feb. 9, 2026; Accepted: Feb. 26, 2026; Published: Mar. 4, 2026

Forensic Medical Assessment of Medical Care Defects in Obstetrics and Pediatrics
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJ. K. Kalandarov, U. S. Kuziev
Department of Pathomorphology, Urgench State Medical Institute, Urgench, Uzbekistan
Correspondence to: J. K. Kalandarov, Department of Pathomorphology, Urgench State Medical Institute, Urgench, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Defects in medical care provided in obstetric and pediatric practice remain a major clinical, social, and forensic medical problem. Errors at diagnostic, therapeutic, surgical, and organizational stages may result in severe iatrogenic complications, including maternal and pediatric mortality [13,20]. Objective: To analyze the frequency, structure, and forensic medical characteristics of medical care defects in obstetrics and pediatrics and to improve criteria for their commission forensic medical assessment. A retrospective forensic medical analysis was conducted based on 250 commission forensic medical examination reports from the Republican Scientific-Practical Center of Forensic Medical Examination and its regional branches (Tashkent, Khorezm, Bukhara, and the Republic of Karakalpakstan) for the period 2020-2024. The study included 40 obstetric-gynecological and 32 pediatric cases with confirmed iatrogenic pathology. Clinical documentation, morphological (macroscopic and microscopic), histological, and statistical methods were applied. Medical care defects were most frequently associated with diagnostic errors, delayed emergency care, irrational pharmacotherapy, and non-compliance with clinical standards [12,18,19]. In pediatric practice, iatrogenic pathology accounted for 6.8% of mortality, while in obstetric practice, defects predominated among patients aged 31-40 years. Morphological examination revealed consistent thanatogenetic patterns, including hypoxic-ischemic lesions, cerebral and pulmonary edema, polyorgan failure, and infectious complications [14,17]. Medical care defects in obstetrics and pediatrics represent a significant source of iatrogenic pathology. Comprehensive forensic medical assessment based on clinical-morphological analysis improves the objectivity of expert conclusions and contributes to prevention of adverse outcomes.
Keywords: Forensic medical examination, Obstetrics, Pediatrics, Iatrogenesis, Medical care defects, Malpractice, Thanatogenesis
Cite this paper: J. K. Kalandarov, U. S. Kuziev, Forensic Medical Assessment of Medical Care Defects in Obstetrics and Pediatrics, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 913-915. doi: 10.5923/j.ajmms.20261603.14.
Article Outline
1. Introduction
- Obstetrics and pediatrics are among the most responsibility-intensive medical specialties, as they directly affect maternal and child health outcomes. Defects in medical care at any stage can lead to irreversible pathological changes and fatal outcomes. International evidence suggests that preventable medical errors remain a substantial contributor to adverse hospital outcomes and mortality [13]. Children and newborns are particularly vulnerable due to anatomical and physiological immaturity, whereas obstetric patients face increased risks related to pregnancy-associated complications, including thromboembolic events [1,11]. In this context, forensic medical examination (FME) plays a key role in identifying defects in medical care, establishing causal relationships, clarifying thanatogenetic mechanisms, and providing evidence-based expert conclusions in malpractice litigation and quality-improvement initiatives [12,18,19]. Despite ongoing improvements in clinical guidelines, cases of iatrogenic pathology in obstetric-gynecological and pediatric care remain relevant in many healthcare systems [2,5,16].
2. Materials and Methods
- Study design and setting: A retrospective forensic medical study was conducted using commission-based FME materials collected in 2020-2024 from the Republican Scientific-Practical Center of Forensic Medical Examination and its regional branches (Tashkent, Khorezm, Bukhara, and the Republic of Karakalpakstan) [3]. Study sample: A total of 250 commission cases were reviewed. The analytical cohort comprised 72 cases with confirmed iatrogenic pathology, including 40 obstetric-gynecological cases and 32 pediatric cases involving children under five years.Data sources: Expert conclusions were derived from medical records, emergency service documentation, inpatient charts, operative reports (when applicable), autopsy protocols, and histological archives.Methods of analysis: The following methods were used: (1) clinical and anamnestic analysis; (2) forensic medical assessment; (3) macroscopic and microscopic morphological assessment; (4) forensic histological examination; (5) comparative evaluation of clinical and morphological findings; and (6) statistical analysis using Pearson's chi-square (χ²) test.Ethical considerations: The study used archival expert documentation and anonymized data. Ethical principles of medical practice in obstetrics and gynecology were considered in the interpretation of findings [20].
3. Results
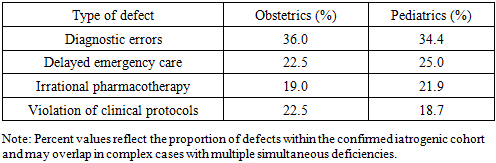
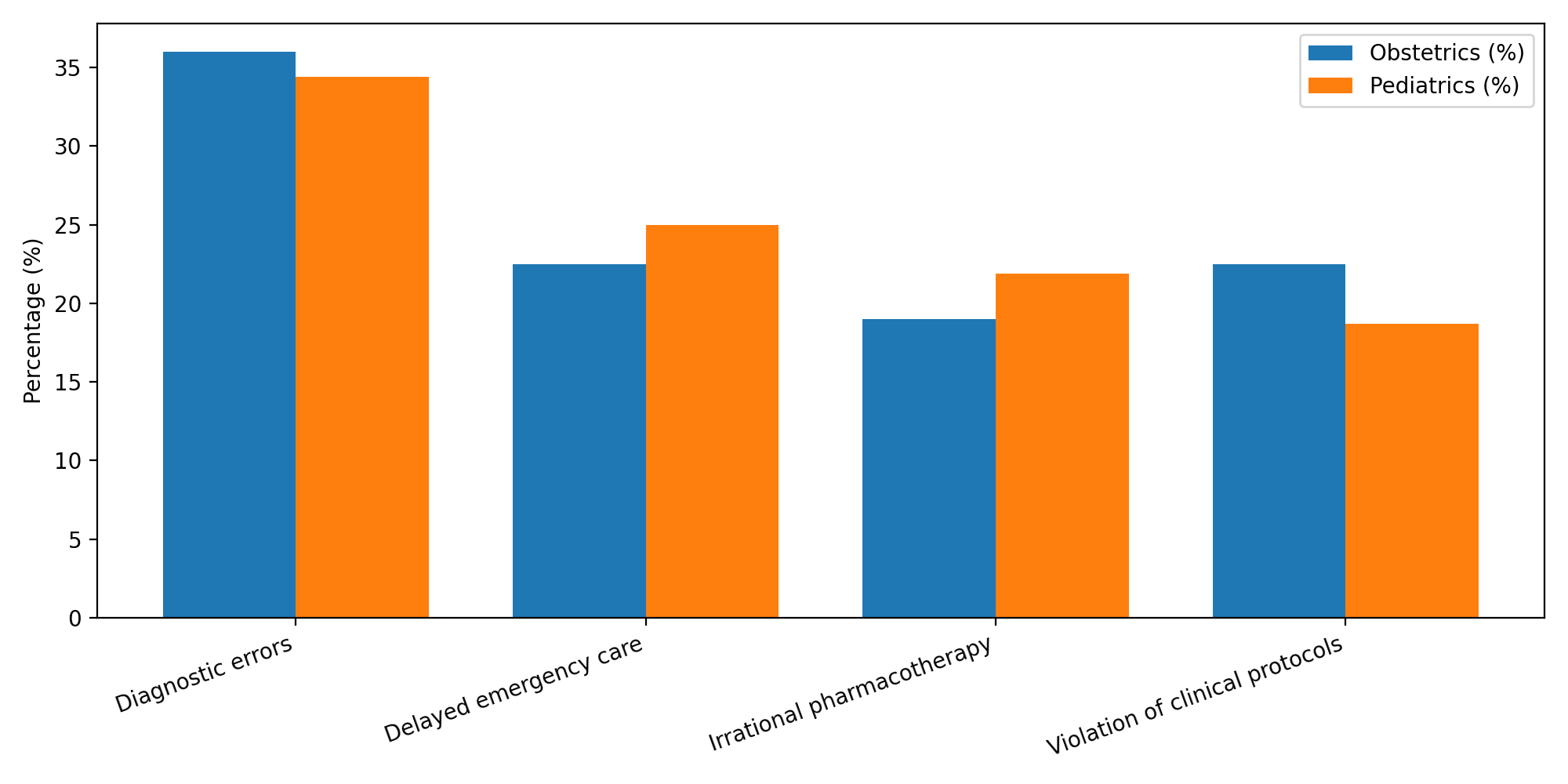
- The analysis demonstrated that defects in medical care were most often related to: diagnostic errors, delayed emergency care, irrational pharmacotherapy, and violations of clinical protocols/standards. In pediatric practice, iatrogenic pathology accounted for 6.8% of mortality, predominantly due to delayed diagnosis and inadequate emergency management. In obstetric and gynecological practice, the highest frequency of defects was observed among patients aged 31-40 years, with differences between regions potentially reflecting variability in access to timely specialist care and adherence to standards. Morphological examination revealed a unified set of thanatogenetic mechanisms across both groups, including hypoxic-ischemic injury, cerebral and pulmonary edema, polyorgan failure, septic complications, and, in some cases, anaphylactic reactions [17,19].
|
 | Figure 1. Suggested algorithm for commission-based forensic medical assessment of medical care defects |
4. Discussion
- The findings indicate that defects in medical care in obstetrics and pediatrics share common etiological patterns and thanatogenetic mechanisms. Subjective factors (insufficient clinical vigilance, delayed decision-making) and organizational issues (limited resources, delayed referral pathways) often contribute to adverse outcomes. These observations are consistent with published forensic analyses of medical errors in obstetric-gynecological practice [12,18,19] and with broader patient safety concepts promoted internationally [13]. From a clinical perspective, obstetric patients may develop rapidly progressing critical conditions (e.g., hemorrhage, hypertensive disorders, and thromboembolic complications) requiring prompt risk stratification and adherence to protocols [1,11]. In pediatrics, the short diagnostic window and age-specific physiology make timely recognition of deterioration essential; thus, delays and inadequate emergency actions have a disproportionately severe impact. Morphological and histological criteria, including hypoxic-ischemic lesions, edema, multi-organ failure, and infectious/septic changes, provide objective evidence for expert conclusions and facilitate causality assessment [14,17]. The integration of clinical documentation with morphological verification increases the validity of commission-based FME reports and supports prevention strategies aimed at reducing iatrogenic pathology [2,5,16].
5. Conclusions
- 1. Defects in medical care in obstetrics and pediatrics represent a significant source of iatrogenic pathology.2. Diagnostic errors and delayed emergency interventions are the leading contributors to adverse outcomes.3. Morphological and histological criteria are essential components of forensic medical assessment and causal reasoning.4. Integrated commission-based forensic evaluation improves objectivity and helps guide preventive measures.
6. Practical Recommendations
- 1. Strengthen continuous professional training of obstetric, pediatric, and neonatal healthcare providers.2. Ensure strict adherence to clinical protocols and standards with routine audits.3. Improve interdisciplinary cooperation between clinicians and forensic experts to facilitate feedback loops.4. Implement structured expert assessment algorithms (Figure 1) in routine commission-based forensic practice.