Ismailova M. U., Ashurova D. T.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
A total of 43 children aged 3–12 years were examined. The patients were divided into two groups. The main group (n=20) received combined general anesthesia with fentanyl, propofol, and sevoflurane. The control group (n=23) received general anesthesia based on fentanyl and propofol. Hemodynamic parameters including heart rate (HR), mean arterial pressure (MAP), ejection fraction (EF), and stroke volume (SV) were evaluated at different stages of anesthesia. The depth of anesthesia was assessed using bispectral index (BIS) monitoring at the stages of premedication, induction, intubation, traumatic stage of surgery, and completion of the operation. Analysis of hemodynamic indicators and BIS values demonstrated greater stability of cardiovascular parameters and more controlled anesthesia depth in the group receiving fentanyl, propofol, and sevoflurane. The combined use of low-dose fentanyl with propofol and sevoflurane provided a smoother clinical course and more stable general anesthesia compared with the standard technique based on fentanyl and propofol.
Keywords:
Anesthesia, Opioid, Fentanyl, Hip joint, Arthroplasty
Cite this paper: Ismailova M. U., Ashurova D. T., Low-Opioid Anesthesia Using Fentanyl During Hip Arthroplasty in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 907-912. doi: 10.5923/j.ajmms.20261603.13.
1. Introduction
Due to the high prevalence, congenital anomalies of the musculoskeletal system represent a complex medical and social problem. According to various authors, the incidence ranges from 47 to 237 cases per 1,000 of the pediatric population. Congenital diseases and developmental anomalies of the lower extremities account for up to 31% of disabling pediatric pathology, and by the age of 4 years the level of disability increases 2.5 times. Surgical correction makes it possible to restore the functional state of the limb and ensures the development of its absent or lost function [1].The extent and traumatic nature of orthopedic surgical interventions in children require effective and safe analgesia [2,4].From this perspective, the inclusion of opioids as a specific component of balanced anesthesia is widely accepted. Fentanyl is an important opioid, and its use during surgical interventions is a necessary component influencing pain reduction [3]. Fentanyl is similar to other μ-opioid receptor agonists in its pharmacological effects, which include analgesia, euphoria, sedation, nausea, and respiratory depression [5].The evaluation of fentanyl efficacy should be interpreted with caution, since bioavailability varies depending on dosage [5,6]. There are important reports by authors regarding the doses of fentanyl used in pediatric anesthesiology, associated with the presence of severe complications in case of drug overdose, the main of which is dose-dependent respiratory depression in the postoperative period, sometimes leading to catastrophic consequences [7,8,9].Even high doses of opioid analgesics do not affect nociceptive pain structures and do not block them [10,11].Certain advantages are associated with the combination of opioid analgesics with inhalational anesthetics [11]. Inhalational volatile anesthetics modify consciousness from the stage of analgesia (confusion) to the surgical stage of anesthesia (complete loss of consciousness). Some researchers believe that sevoflurane in pediatric anesthesiology prevents the development of post-anesthetic agitation syndrome with prolongation of the drug-induced sedation phase and reduction of hyper sympathicotonia. Sevoflurane is widely used for maintenance and even induction of general anesthesia both in the operating room and outside it [12].In this regard, the issues of analgesia in patients using the opioid analgesic fentanyl in combination with sevoflurane are relevant.The aim of the study was to improve the quality of anesthesia through the combined use of low doses of the opioid fentanyl during hip arthroplasty in children.
2. Materials and Methods
A prospective study included 43 patients (3–12 years old, mean age 5.7±0.63) with congenital hip dislocation who were operated on in the Children’s Multidisiplinary Clinic of Tashkent State Medical University. The objective status of the patients according to ASA corresponded to class II–III. The inclusion criteria were as follows: 1) age of patients from 3 to 12 years; 2) presence of informed consent for surgical intervention; 3) pathological hip dislocation. Exclusion criteria: 1) pathological hip dislocation; 2) patients suffering from severe systemic diseases.Table 1. Distribution of children by groups, gender, duration of surgery and anesthesia
 |
| |
|
In both groups, the following drugs were used for premedication: atropine sulfate 0.1% – 0.01 mg/kg; ketamine 5% – 1 mg/kg; sibazone 0.5%; diphenhydramine 1% – 0.1 mg/kg.For anesthetic management of the surgical intervention, combined general anesthesia based on fentanyl, propofol, and sevoflurane was used in the absence of contraindications. Forty minutes before surgery, dexamethasone 0.4% – 0.15 mg/kg was administered intravenously.For induction of general anesthesia, intravenous boluses were administered sequentially: propofol 2 mg/kg, fentanyl 0.005% 3–2.5 µg/kg, arduan 0.2% – 0.06 mg/kg.Maintenance of general anesthesia: insufflation of sevoflurane at a dose of 1.5–1 MAC, fentanyl ½ and 1/3 of the induction dose.In the control group, induction was performed with propofol 3 mg/kg and fentanyl 5 mg /kg, arduan 0.06 mg/kg.Maintenance of anesthesia was carried out with propofol 100–150 µg/kg/min as a continuous infusion and fentanyl ½ and 1/3 of the induction dose.The following parameters were studied: heart rate (HR), mean arterial pressure (MAP), cardiac index (CI), ejection fraction (EF), and circumferential shortening velocity (CSV).The depth of anesthesia was studied using BIS monitoring on the UM 300 “Yutas” device at the following stages: premedication, induction, intubation, traumatic stage, and end of surgery.
3. Results and Discussion
The analysis of this parameter in patients of Group 1, when using the selected method of general anesthesia, was compared with average physiological data. The analysis of this parameter at the stages of anesthesia and surgery showed that at the premedication stage a significant increase was noted (by 12.9% from baseline), which was regarded as a slight increase not requiring correction. At the induction stage, a more pronounced increase was observed (by 15% from baseline). The main stage of the operation, being the most painful, was characterized by a tendency toward a decrease in heart rate (by 8% from baseline), while remaining within average physiological limits. The final stage of anesthetic management was considered quite distinctive, when the heart rate was slightly reduced (by 9.1% from baseline), but in most cases did not require deepening of anesthesia.Thus, it can be noted that the heart rate indicator at almost all stages of surgical treatment of orthopedic pathologies in children was evenly distributed within average physiological parameters.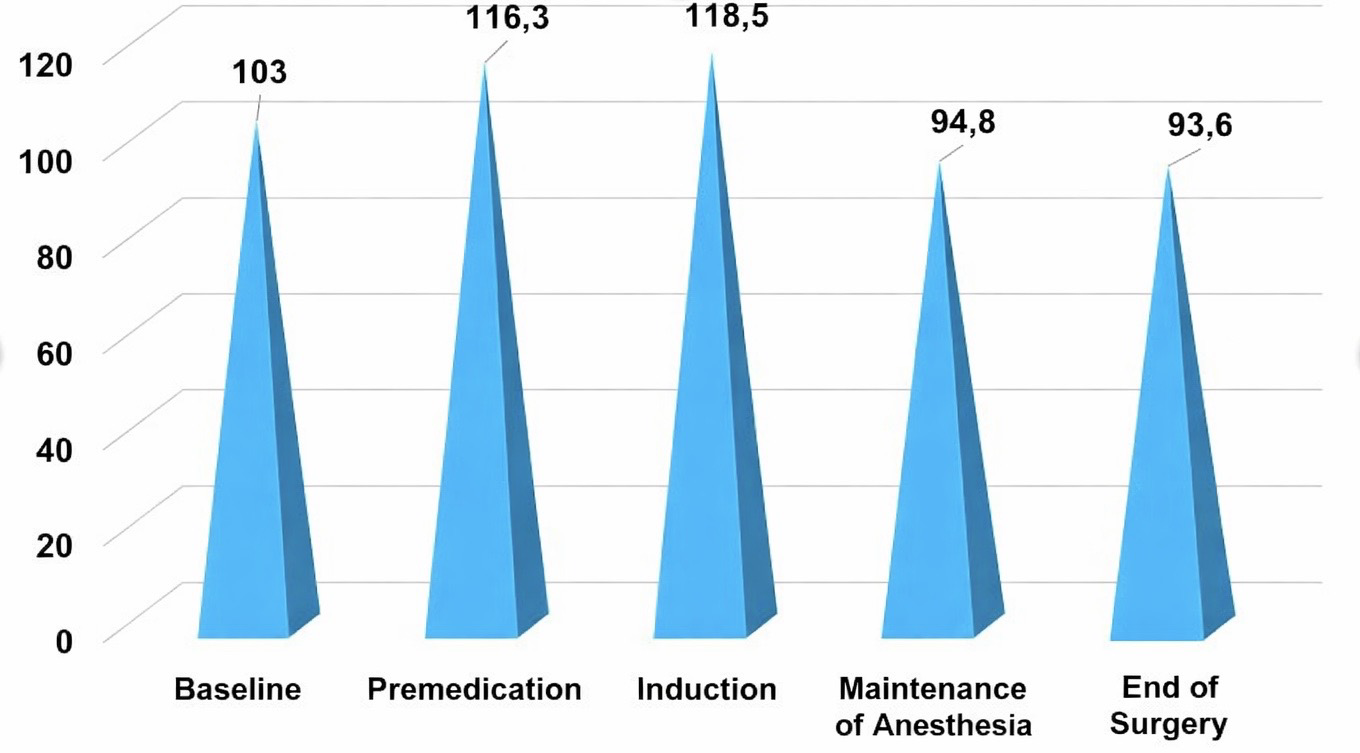 | Figure 1. Heart rate indicators of group 1 patients at the stages of anesthesia |
Another representative among hemodynamic parameters was the level of mean dynamic pressure (MDP), characterizing the cumulative difference between systolic and diastolic arterial pressures. In the examined patients of Group 1, with the selected general anesthesia, no significant provoking deviations of this parameter were noted. At the initial stage of anesthetic management, its values were recorded as balanced with standard indicators and were regarded as average physiological. At the premedication stage, MDP parameters relatively decreased (by 1.3% from baseline), which did not require correction. The induction stage proceeded smoothly; however, an increase in the considered parameter (by 2% from baseline) excluded the use of radical pharmacological correction methods. A uniform decrease in MDP at the main stage of anesthesia maintenance (by 11.4% from baseline) did not change the general condition of patients and was regarded as average physiological. Upon completion of all stages of surgical treatment and anesthetic management, only a slight decrease in MDP relative to the previous stage was noted (by 3.6%), but it remained elevated by 0.44% from baseline. It can be noted that changes in MDP during all stages of anesthesia did not undergo significant alterations, positively characterizing the applied method of general anesthesia.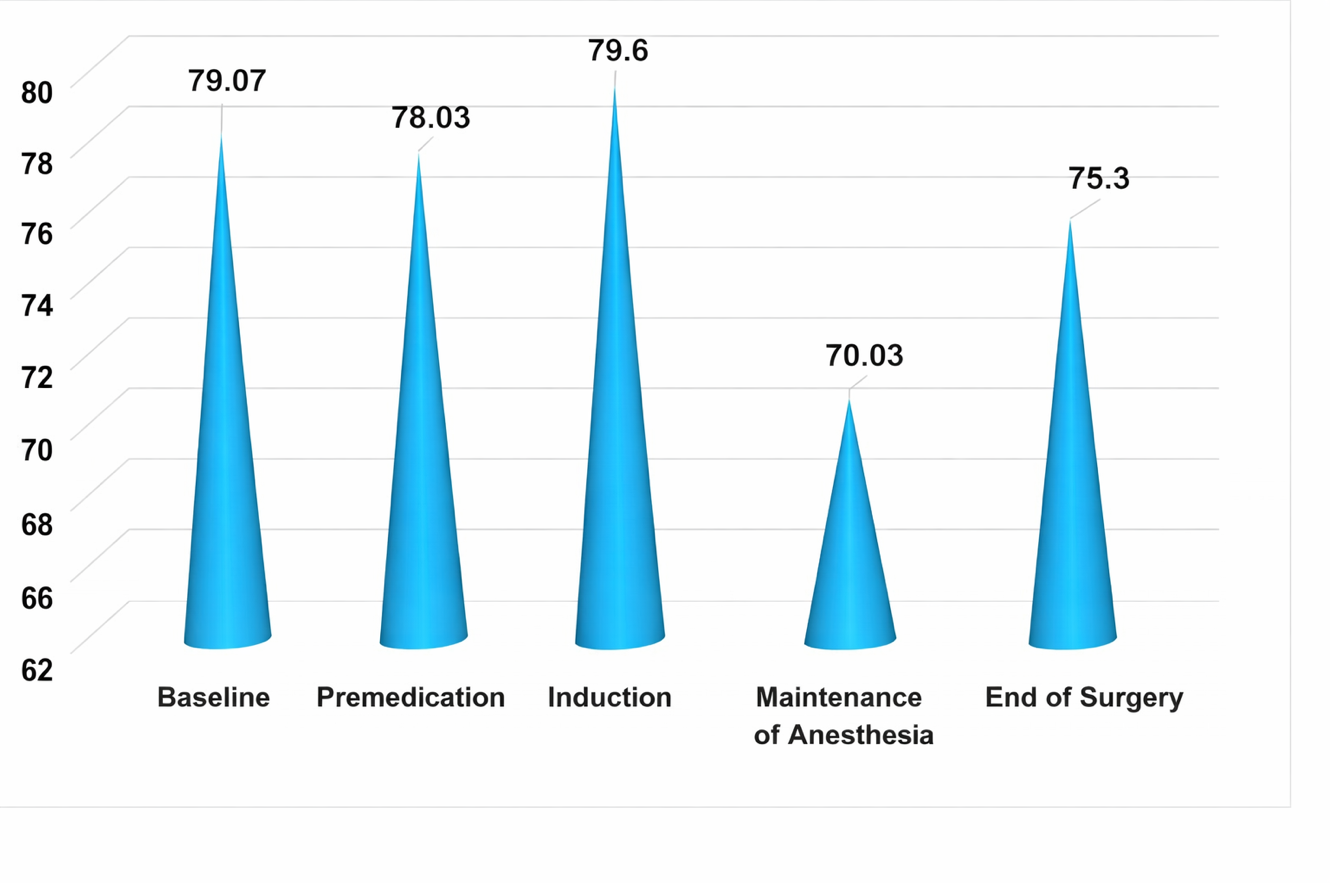 | Figure 2. Changes in MDP of group 1 at various stages of the study |
Thus, the studies conducted during anesthetic management in Group 1 patients were analyzed separately at each stage. Considering the baseline BIS index values (78.69), it can be noted that already at the premedication stage deep sedation was registered in patients, confirming the adequacy of the anesthesia method used. At the induction stage, a sufficient decrease in the indicator was observed (by 29.15% from baseline), reflecting a deep level of anesthesia with a low probability of consciousness. The most traumatic period of anesthetic management is particularly distinguished by the lowest BIS index value (by 33.68% from baseline) with this type of general anesthesia in children of Group 1. Gradual completion of the operation, coordinated reduction of anesthetic doses and their complete discontinuation were characterized by a relative increase in the BIS index (by 23.05% from the previous stage), but it remained reduced by 18.4% from baseline. The use of this research method (Fig. 3) made it possible to selectively control the course of anesthesia and brain functioning at all stages of surgical treatment, which in turn prevented the negative effects of anesthesia, allowing possible therapeutic decisions in ineffective cases. 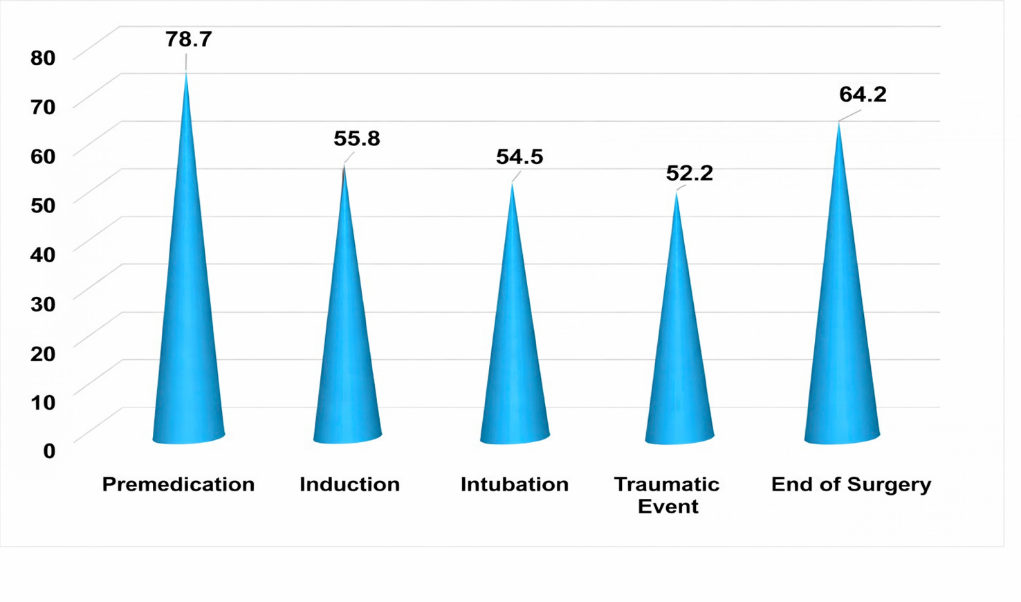 | Figure 3. Changes in BIS indicators in group 1 (n=20) at different stages of the study |
However, when using this anesthetic method, no negative aspects of anesthesia were observed; all stages proceeded quite smoothly and flawlessly.A sufficiently detailed study of hemodynamic parameters was also carried out in patients of Group 2 (23) when using the standard method of analgesia (fentanyl + propofol) during orthopedic operations. Considering the obtained heart rate values (normally 98.1 beats per minute) at the stages of anesthetic management, a fairly pronounced difference in fluctuations of this parameter was noted when compared with the same parameter in Group 1. Already at the initial stage of surgical treatment, a noticeable increase in the parameter was observed (by 12.2% above the standard), which created certain caution in further actions. The premedication stage was characterized by a similar increase in heart rate relative to baseline values by 11.74% and by 28.38% above the standard, respectively. The most significant changes occurred at the induction stage, when a marked increase in heart rate was registered (by 28.16% from baseline; by 43.8% above the standard), which required corrective pharmacological intervention and adjustment of anesthetic administration. This, in turn, allowed a sufficiently significant decrease in the parameter at the main stage of anesthesia, although its increase (by 2% from baseline) also required caution. At the stage of completion of the surgical intervention and anesthetic management, an objective increase in heart rate was recorded (by 4.8% from the previous stage), yet it remained somewhat elevated by 4.86% from baseline. It should be noted that this type of analgesia requires a special approach and caution during orthopedic operations, with regulation of the hemodynamic capabilities of the body.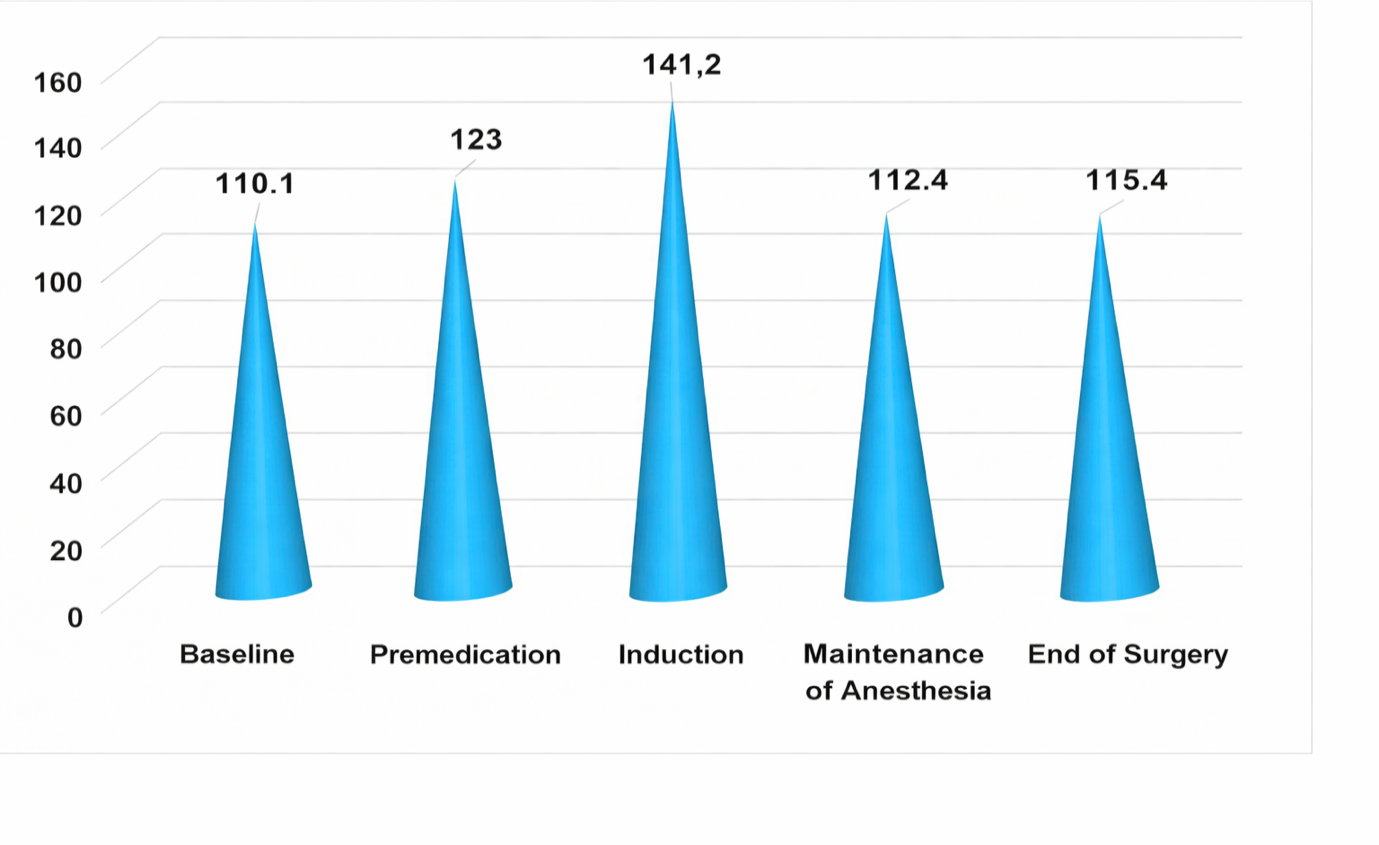 | Figure 4. Changes in heart rate in group 2 patients at different stages of the study |
Confirmation of the above was noted in the analysis of mean arterial pressure in this group of patients, conducted in parallel with heart rate at all stages of anesthesia. The range of MDP parameters at the stages of anesthesia required certain correction methods during surgical treatment. The baseline state (75.83 mmHg normally) was relatively elevated (by 5.32% above normal), which required close monitoring of the patient’s condition and hemodynamic parameters. At the premedication stage, an increase in MDP was recorded (by 11.7% from baseline), considered as a reaction of the cardiovascular system. Moreover, at the induction stage, a further increase (by 28.2% from baseline) required deepening of anesthesia. 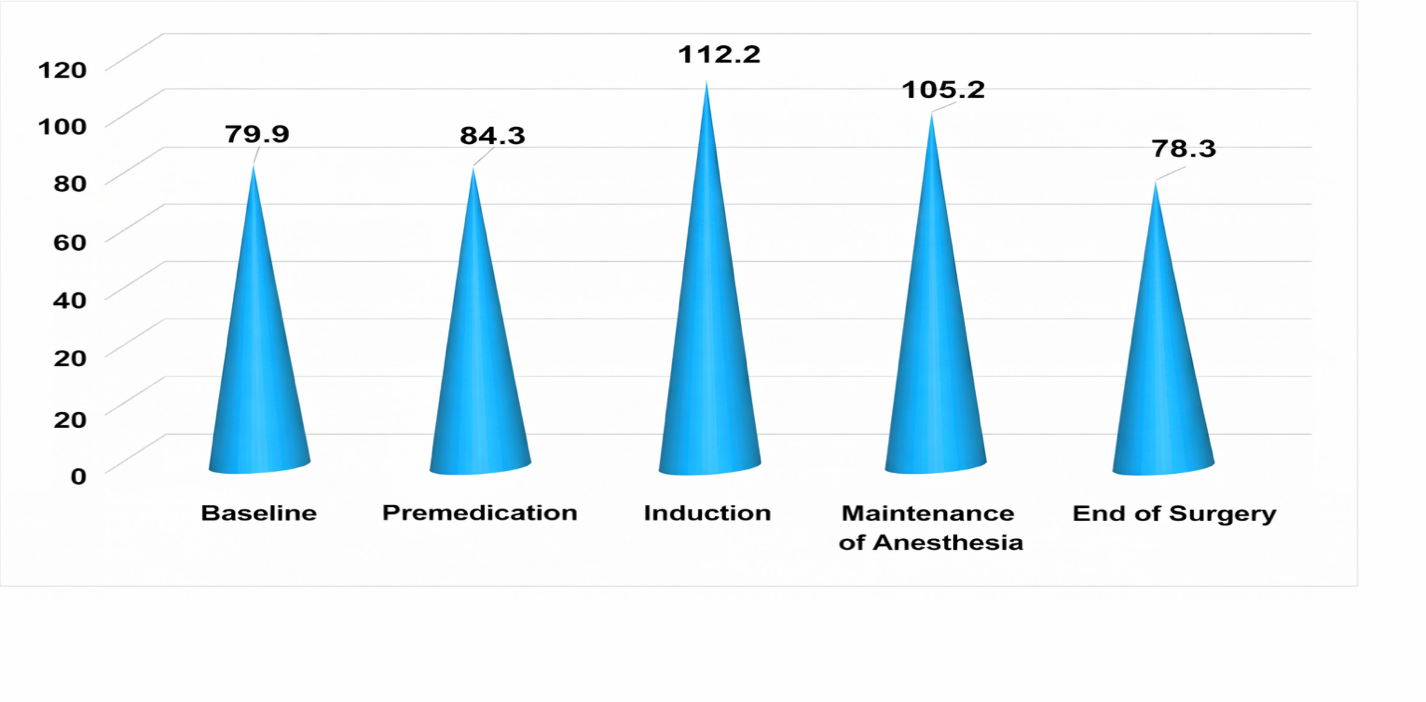 | Figure 5. Changes in MDP in group 2 at different stages of the study |
Thus, at the stage of anesthesia maintenance, the initiation of correction of hemodynamic disturbances made it possible to relatively level MDP values, with its increase by 2% from baseline. The continuation of corrective hemodynamic methods resulted in a slight increase in MDP already at the end of surgery; upon completion of anesthetic management (by 4.8% from baseline), the level of the parameter was increased by 2.6% from the previous stage. Thus, the use of standard anesthesia methods in the second group of patients was characterized by pronounced fluctuations of the studied parameters.The simultaneous study and assessment of the depth of general anesthesia and sedation in these patients during standard general anesthesia using BIS index monitoring made it possible to determine the doses of the drugs used. In this group of patients (23), the BIS index values at the premedication stage (77.91 units) corresponded to deep sedation. However, the use of anesthetic management methods at the induction stage revealed a certain decrease in the BIS index (by 20.60% from the previous stage), considered undesirable, especially since during intubation this indicator was lower (by 22.66% from the premedication stage) than desired. Even the use of corrective methods did not allow regulation of the studied parameter at an adequate level, and already at the anesthesia maintenance stage a progressive decrease in the BIS index was noted (29.16% from the premedication stage), which logically required changes in anesthetic administration settings and correction of the developing changes. Only at the stage of completion of the operation, during the awakening period, a relative increase in the BIS index level was observed (by 3.93% from the previous stage). The data are presented in Fig. 6.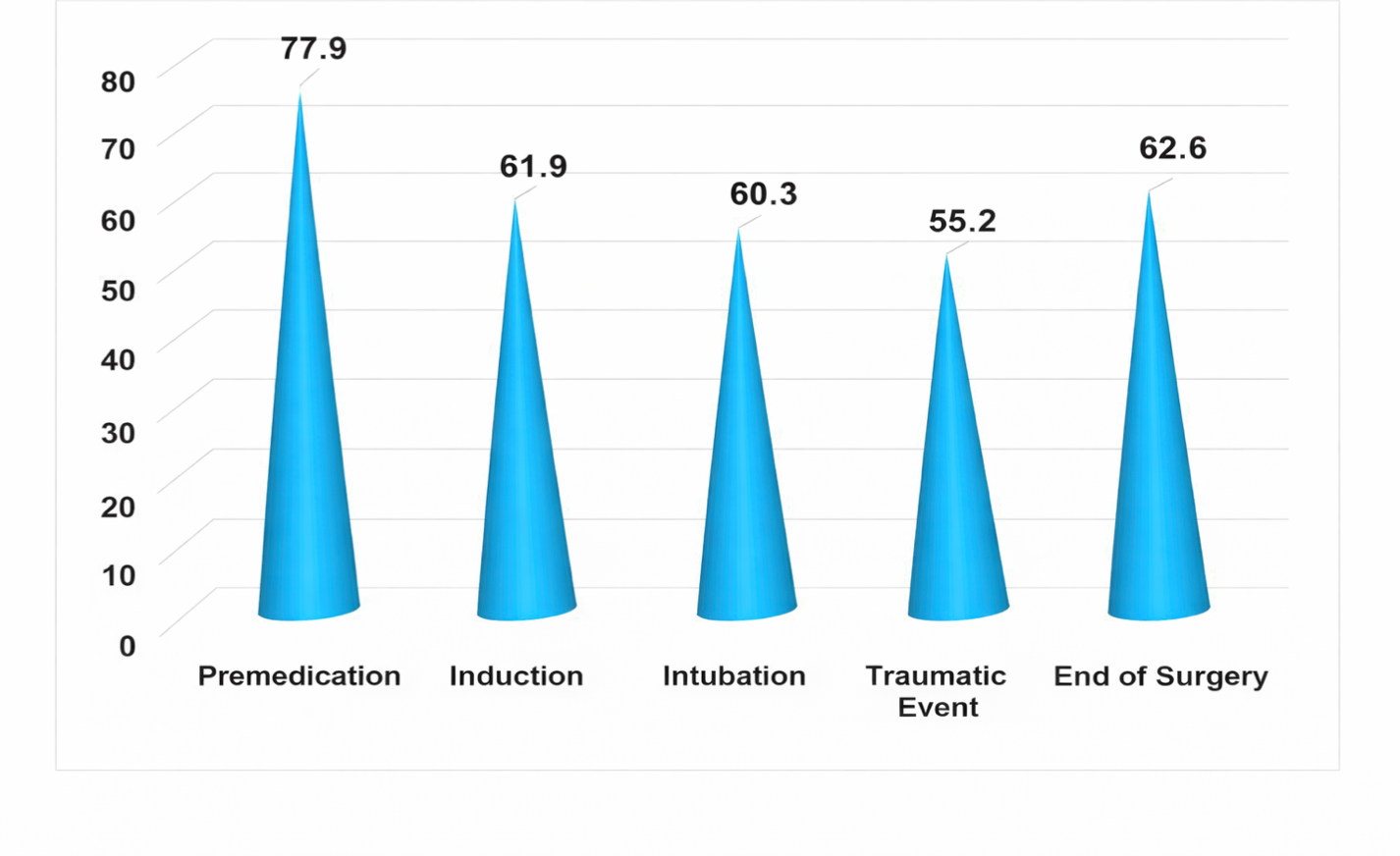 | Figure 6. Changes in BIS index in Group 2 (n=23) at the stages of the study |
Thus, the need for caution in implementing this anesthetic management method in this group of patients remained significant at all stages of surgical treatment.
4. Conclusions
1. Combined anesthesia based on low doses of fentanyl, sevoflurane, and propofol is characterized by a smooth clinical course and maintenance of stable systemic hemodynamic parameters in children undergoing hip arthroplasty.2. The BIS index of general anesthesia based on sevoflurane, fentanyl, and propofol, determined by EEG studies and ranging within 55.75–64.21, allows regulation of anesthetic drug doses and avoidance of episodes of excessively deep and superficial anesthesia.3. Combined anesthesia based on the inhalational anesthetic sevoflurane in combination with fentanyl and propofol proceeds with minor changes in central hemodynamic parameters, without significant changes in stroke volume and cardiac output.
References
| [1] | Agzamkhodjaev T.S., Ismailova M.U. Comparative assessment of variants of multicomponent inhalational anesthesia in pediatric orthopedics // Proceedings of the International Conference of Anesthesiologists and Resuscitators. – Tashkent, 2019. – P. 108. |
| [2] | Alexandrovich Yu.S., Barsukova I.M., Bogomolov B.N., Vartanova I.V., Golub I.V., Korostelev Yu.M., Luft A.V., Luft V.M., Miroshnichenko A.G., Obrezan A.G., Polushin Yu.S., Pshenisnov K.V., Shlyk I.V. Fundamentals of Anesthesiology and Resuscitation: Textbook for Medical Universities. 2nd ed., revised and supplemented / Edited by Yu.S. Polushin. – Saint Petersburg: Eco-Vector, 2020. – P. 68–79. |
| [3] | Arbak D.M., Abuzarova G.R., Alekseeva G.S. Opioid analgesics in clinical medicine of the 21st century // Russian Journal of Pain. – 2014. – No. 2. – P. 39–50. |
| [4] | Belousov D.Yu., Afanasyeva E.V., Efremova E.A. Comparative assessment of the economic effectiveness of modern inhalational anesthetics // Quality Clinical Practice. – 2014. – No. 2. – P. 3–20. |
| [5] | Bragina N.V., Gorbachev V.I., Netesin E.S. On the choice of fentanyl dose in pediatric anesthesiology // Anesthesiology and Resuscitation. – 2021. – No. 2. – P. 56–86. |
| [6] | Gubaidullin R.R., Belousov D.Yu., Cheberda A.E. Clinical and economic evaluation of the use of inhalational anesthetics // Bulletin of Anesthesiology and Resuscitation. – 2017. – Vol. 14, No. 5. – P. 8–19. |
| [7] | Zozulya M.V., Lenkin A.I., Kurapeev I.S., Saiganov S.A., Lebedinsky K.M. Effectiveness of lidocaine as an adjuvant to opioid analgesia in patients after planned cardiac surgery // Anesthesiology and Resuscitation. – 2021. – No. 2. – P. 67–73. |
| [8] | Kozyrev A.S., Alexandrovich Yu.S., Zaletina A.V., et al. Comparative assessment of anesthesia with desflurane and sevoflurane during surgical correction of spinal cord injury in children // Orthopedics, Traumatology and Reconstructive Surgery of Childhood. – 2018. – Vol. 6(3). – P. 47–55. DOI: 10.17816/PTORS6347-55. |
| [9] | Kolesnikov Yu.A. Central and peripheral mechanisms of mu-opioid analgesia and tolerance // Bulletin of Anesthesiology and Resuscitation. – 2020. – Vol. 17, No. 1. – P. 9–20. |
| [10] | Ovezov A.M., Pivovarova A.A., Khalimov M.R. Methodological aspects of the use of sevoflurane in modern anesthesiology. Literature review // Bulletin of Intensive Therapy named after A.I. Saltanov. – 2020. – No. 4. – P. 74–87. DOI: 10.21320/1818-474X-2020-4-74-87. |
| [11] | Yusupov A.S., Ismailova M.U. Changes in central hemodynamic parameters during orthopedic operations in children // Pediatrics. – Tashkent, 2022. – No. 4. – P. 125–130. |
| [12] | Ismailova M.U., Ashurova D.T. Dynamics of Stress Hormone Levels with Low-Opioid Anesthesia During Thoracoplasty in Children // American Journal of Medicine and Medical Sciences. – 2025. – 15(4): 1201–1205. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML