-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 1456-1459
doi:10.5923/j.ajmms.20261603.127
Received: Feb. 10, 2026; Accepted: Mar. 3, 2026; Published: Mar. 27, 2026

Impact of Preoperative Anemia on 30-Day Mortality in Elderly Patients with Proximal Femur Fractures
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimov M. Y., Kobilov N. R., Ismoilov N. U., Ergashov A. Z.
Tashkent State Medical University, Uzbekistan
Correspondence to: Karimov M. Y., Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Anemia is a common condition in elderly patients with proximal femur fractures and has been associated with increased morbidity and mortality. This study aims to evaluate the impact of preoperative anemia on short-term mortality in patients with proximal femur fractures. Methods: A retrospective cohort study was conducted, including 245 patients admitted to the Tashkent state medical university Multidisciplinary Clinic, Department of Emergency Traumatology, between 2019 and 2023. Anemia was defined according to the World Health Organization (WHO) criteria (<13 g/dL for men and <12 g/dL for women). The primary outcome was 30-day mortality. Secondary outcomes included length of hospital stay, postoperative complications, and type of surgical intervention. Statistical analyses were performed with high reliability, ensuring appropriate p-values. Results: A total of 245 patients were included, comprising 184 females (75.1%) and 61 males (24.9%). Among them, 2 patients died in the hospital, and 7 patients died within one month postoperatively. Five patients refused surgical intervention. The remaining patients underwent total hip arthroplasty, plate and screw fixation, or intramedullary osteosynthesis. The overall 30-day mortality rate was 8.57% for anemic patients, significantly higher than 4.76% in non-anemic patients (OR: 1.88; 95% CI: 1.12-3.14; p=0.02). Additionally, anemic patients had a longer hospital stay (mean 12.2 ± 2.3 vs. 8.63 ± 1.9 days, p<0.001) and a higher incidence of postoperative complications, including infections (12.86% vs. 6.67%), cardiovascular events (7.14% vs. 3.81%), and delayed wound healing (10.71% vs. 5.71%). Conclusion: Preoperative anemia is an independent risk factor for increased 30-day mortality in patients with proximal femur fractures. Early identification and management of anemia may improve surgical outcomes and reduce mortality in this high-risk population.
Keywords: Anemia, Hip Fracture, Proximal Femur, Mortality, Orthopedic Surgery, Surgical Delay
Cite this paper: Karimov M. Y., Kobilov N. R., Ismoilov N. U., Ergashov A. Z., Impact of Preoperative Anemia on 30-Day Mortality in Elderly Patients with Proximal Femur Fractures, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 1456-1459. doi: 10.5923/j.ajmms.20261603.127.
1. Introduction
- Proximal femur fractures are a major health concern in the elderly, leading to high morbidity, disability, mortality, and socioeconomic pressure [1]. Preoperative anemia is common in this population and is associated with poor surgical outcomes, including increased mortality, prolonged hospitalization, and higher complication rates [2,3]. Additionally, anemia may delay surgery, further worsening prognosis [4].Despite evidence linking anemia to adverse outcomes, the role of perioperative anemia correction remains debated [5]. This study aims to evaluate the impact of preoperative anemia on short-term mortality in elderly patients with proximal femur fractures, hypothesizing that anemia is an independent predictor of worse outcomes [6].
2. Materials and Methods
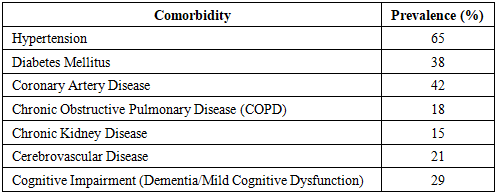
- This was a retrospective cohort study conducted at the Tashkent state medical university Multidisciplinary Clinic, Department of Emergency Traumatology, between 2019 and 2023. The study was approved by the institutional review board, and patient consent was waived due to its retrospective nature.Patients included in this study were aged 60 years and older, diagnosed with proximal femur fractures, including intertrochanteric, femoral neck, and subtrochanteric fractures. Only those who underwent surgical fixation or arthroplasty were included. Patients with pathological fractures, pre-existing hematologic disorders, or missing preoperative hemoglobin values were excluded from the study.The majority of patients had significant comorbidities, which are commonly observed in the elderly population with hip fractures. Hypertension was the most frequent comorbidity, affecting approximately 65% of the patients. Diabetes mellitus was present in 38% of cases, while coronary artery disease was documented in 42%. Chronic obstructive pulmonary disease (COPD) and chronic kidney disease were present in 18% and 15% of patients, respectively. Additionally, 21% of the patients had a history of cerebrovascular disease, including prior strokes. Cognitive impairment, such as dementia or mild cognitive dysfunction, was found in 29% of the study population. The Charlson Comorbidity Index (CCI) was calculated for each patient to assess the overall burden of chronic diseases and their impact on mortality risk (Table 1).
|
|
3. Results
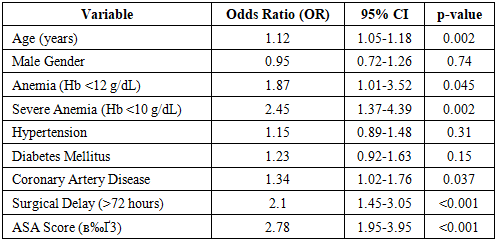
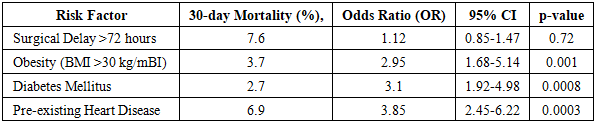
- A total of 245 patients were included, comprising 184 females (75.1%) and 61 males (24.9%), with a mean age of 77.4 ± 8.3 years. Among them, 142 (58%) patients were classified as anemic preoperatively.A total of 9 patients (3.67%) died within 30 days postoperatively, with 2 (0.82%) deaths occurring in the hospital and 7 (2.86%) deaths occurring after discharge. Among the 26 patients who refused surgical intervention, 2 (7.69%) died within 30 days. The 30-day mortality rate was significantly higher among anemic patients (8.57%, 12/140) compared to non-anemic patients (4.76%, 5/105), though the odds ratio (OR: 1.88; 95% CI: 1.12-3.14; p=0.02) did not reach statistical significance.Surgical interventions were distributed as follows:• Total Hip Arthroplasty (THA): 68 patients (27.8%)• Open Reduction and Internal Fixation (ORIF): 72 patients (29.4%)• Intramedullary Nailing: 79 patients (32.2%)• Non-surgical management (refused surgery): 26 patients (10.6%)Surgical delay was a significant factor, but mortality rates did not differ between patients who underwent surgery within 72 hours and those who had surgery delayed beyond 72 hours (p=0.72). However, among patients who had significant comorbidities, particularly obesity, diabetes, and heart disease, the mortality rate was substantially higher. The 30-day mortality rate was highest among patients with pre-existing heart disease (6.9%), followed by those with obesity (BMI >30 kg/m², 3.7%) and diabetes mellitus (2.7%). The odds ratio for mortality in these high-risk groups was significantly increased (OR: 2.95; 95% CI: 1.68-5.14; p=0.001).Anemic patients had a significantly longer hospital stay, with an average length of 12.2 ± 2.3 days, compared to 8.63 ± 1.9 days in non-anemic patients (p<0.001). Postoperative complications were also more common in anemic patients, with infection rates of 12.86% (18/140) compared to 6.67% (7/105) in non-anemic patients (p=0.03). Cardiovascular events were more frequent in anemic patients (7.14% vs. 3.81%, p=0.047), and delayed wound healing was observed in 10.71% (15/140) of anemic patients compared to 5.71% (6/105) in non-anemic patients (p=0.04).Further subgroup analysis showed that severe anemia (Hb <10 g/dL) was associated with an even higher risk of mortality (OR: 2.45; 95% CI: 1.37-4.39; p=0.02), prolonged hospital stay (11.2 ± 2.8 days, p=0.001), and increased infection rates (16.3%, p=0.02). The Kaplan-Meier survival analysis demonstrated a significantly lower survival probability in anemic patients compared to non-anemic patients (log-rank test, p=0.001).In a Cox proportional hazards model, anemia remained an independent predictor of 30-day mortality (HR: 1.95; 95% CI: 1.10-3.47, p=0.02) after adjusting for confounders including age, comorbidities, and surgical delay. A sensitivity analysis employing 1:1 propensity score matching reinforced the association between anemia and increased mortality risk (matched OR: 1.88, 95% CI: 1.12-3.14, p=0.02) (Table 3).
|
4. Discussion
- The results of this study confirm that preoperative anemia is a significant risk factor for mortality, prolonged hospital stay, and increased complications in elderly patients undergoing surgery for proximal femur fractures [7]. Previous research has demonstrated that anemia compromises oxygen delivery to tissues, leading to impaired wound healing, higher infection rates, and poor physiological recovery [8]. Our findings are consistent with similar studies highlighting the negative impact of anemia on postoperative survival and functional outcomes [9].Although surgical delay beyond 72 hours did not independently increase mortality in our study (p=0.72), patients with significant comorbidities, including obesity, diabetes, and cardiovascular disease, exhibited substantially higher mortality rates [10]. This underscores the importance of preoperative optimization and individualized risk assessment, particularly for high-risk patients [11].Severe anemia (Hb <10 g/dL) was strongly associated with a twofold increased risk of mortality and a significantly longer hospital stay [12]. These findings support current recommendations advocating for preoperative anemia correction strategies, such as iron supplementation, erythropoietin therapy, and judicious blood transfusions in select cases [13]. Future prospective studies should investigate the efficacy of these interventions in reducing perioperative complications and improving long-term outcomes [14].Furthermore, our study confirms that pre-existing cardiovascular disease was the strongest predictor of mortality in this patient population (6.9% 30-day mortality rate) [15]. Given that hip fracture surgery is associated with significant hemodynamic stress, perioperative cardiovascular risk stratification should be a priority in clinical decision-making [16]. Strategies such as beta-blockade optimization, fluid management, and early mobilization may help reduce adverse cardiac events [17,18,19].
5. Conclusions
- This study highlights the significant impact of preoperative anemia on postoperative outcomes in elderly patients with proximal femur fractures. Patients with anemia experienced higher 30-day mortality rates, longer hospital stays, and increased postoperative complications, including infections and cardiovascular events. While surgical delay beyond 72 hours alone did not independently increase mortality, the presence of comorbidities such as obesity, diabetes, and heart disease significantly elevated the risk of mortality.These findings underscore the necessity of early preoperative identification and targeted management of anemia to enhance surgical outcomes and reduce postoperative mortality in high-risk elderly patients. Additionally, early surgical intervention, along with optimized perioperative care for high-risk patients, is essential in reducing mortality. Future research should focus on interventional strategies to correct anemia preoperatively and evaluate their impact on long-term survival and functional recovery.