-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(3): 876-880
doi:10.5923/j.ajmms.20261603.06
Received: Feb. 8, 2026; Accepted: Feb. 25, 2026; Published: Mar. 4, 2026

Association of Matrix Metalloproteinase Gene Polymorphisms with Severity and Functional Outcome of Cardioembolic Stroke in the Uzbek Population
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEgamnazarova Zulaykho Ravshanbek qizi, Musayeva Yulduz Alpisovna
Department of Neurology, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

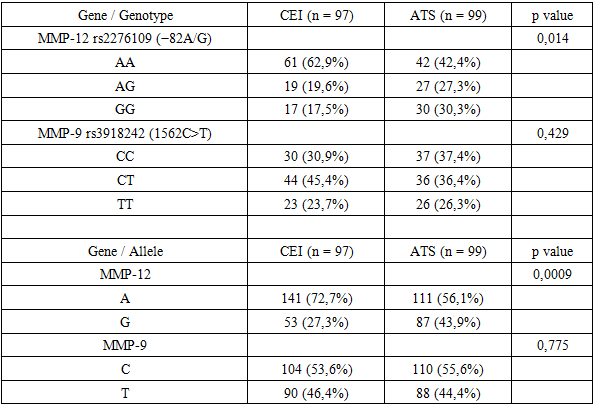
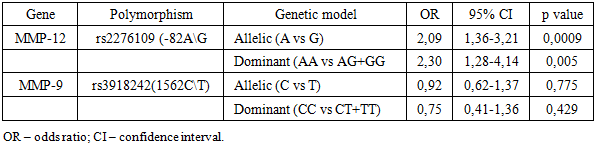
Background: Cardioembolic stroke is characterized by the formation of thromboembolic material in the setting of structural abnormalities of the cardiac chambers or cardiac rhythm disturbances, leading to sudden occlusion of cerebral arteries. Several important studies have addressed stroke epidemiology in Central Asian countries data on genetic profiles and MMP-12 plays an important role mainly in atherosclerosis and ischemic stroke. Despite the available data, the associations of MMP-9 and MMP-12 gene polymorphisms with the development and clinical course of cardioembolic stroke have not been fully investigated, and this issue remains particularly insufficiently studied in the population of Uzbekistan. Methods: The conceptual model of this study was aimed at investigating the clinical course of cardioembolic stroke (CES), the impact of MMP-9 and MMP-12 gene polymorphisms on stroke severity. The study was conducted as a single-center, region-representative, prospective clinical-genetic investigation. The study was conducted in a cohort of patients of Uzbek ethnicity who were admitted to the intensive neurology, intensive care/therapy (ICU), and neurology departments of the clinic of Tashkent State Medical University. A total of 196 patients hospitalized with acute ischemic stroke were enrolled in the study. According to the TOAST classification, 97 patients were classified as having cardioembolic stroke (CES), and 99 patients as having atherothrombotic stroke (ATS). Peripheral venous blood samples were used as biological material for molecular genetic analysis. Blood samples were collected during the acute or early subacute phase of stroke under sterile conditions into EDTA-treated vacuum tubes and processed under laboratory conditions for subsequent analyses. Genomic DNA was isolated using a spin-column (silica-based sorbent column) method in accordance with a standard extraction protocol. Polymorphisms in the promoter regions of the matrix metalloproteinase family genes, namely MMP-9 −1562 C/T (rs3918242) and MMP-12 −82 A/G (rs2276109), were investigated. Results: For the MMP-12 rs2276109 (−82A/G) polymorphism, significant differences in genotype distribution were observed. In the cardioembolic stroke (CES) group, the AA genotype predominated (n = 61, 62.9%), whereas in the atherothrombotic stroke (ATS) group, the AG and GG genotypes were relatively more frequent (n = 19, 27.3% and n = 17, 30.3%, respectively; p = 0.014). The A allele was significantly more frequent in the CES group (n = 141, 72.7% vs n = 111, 56.1%), whereas the G allele was more prevalent in the ATS group (n = 87, 43.9% vs n = 53, 27.3%). According to the association analysis, carriers of the A allele showed an approximately two-fold higher likelihood of developing cardioembolic stroke (OR = 2.09; 95% CI: 1.36–3.21). Furthermore, under the dominant genetic model (AA vs AG + GG), the MMP-12 rs2276109 polymorphism also demonstrated a statistically significant association with cardioembolic stroke (OR = 2.30; 95% CI: 1.28–4.14; p = 0.005), confirming the AA genotype as a potential genetic risk factor for this pathogenic subtype. Conclusion: The high discriminative ability of the NIHSS score on day 1 for predicting a lethal outcome indicating the formation of a distinct “severe clinical phenotype” of cardioembolic stroke. A significant association between the MMP-12 rs2276109 (−82A/G) polymorphism and cardioembolic stroke, especially carriers of the A allele had approximately a two-fold higher risk of developing cardioembolic stroke. In univariate analysis, the AG and GG genotypes showed a protective effect with respect to lethal outcome, whereas the AA genotype was considered a high-risk variant.
Keywords: Cardioembolic stroke, Matrix metalloproteinases, MMP-12, MMP-9, Neurological deficit, National institute of health stroke scale, TOAST classification, Uzbek population
Cite this paper: Egamnazarova Zulaykho Ravshanbek qizi, Musayeva Yulduz Alpisovna, Association of Matrix Metalloproteinase Gene Polymorphisms with Severity and Functional Outcome of Cardioembolic Stroke in the Uzbek Population, American Journal of Medicine and Medical Sciences, Vol. 16 No. 3, 2026, pp. 876-880. doi: 10.5923/j.ajmms.20261603.06.
1. Introduction
- Cardioembolic stroke (CES) is the clinical subtypes of ischemic stroke, which occupies a distinct and clinically important position. This phenotype is characterized by the formation of thromboembolic material in the setting of structural abnormalities of the cardiac chambers or cardiac rhythm disturbances, leading to sudden occlusion of cerebral arteries. According to global epidemiological data, cardioembolic stroke accounts for approximately 20–30% of all ischemic strokes and is distinguished by a more severe clinical course, a higher degree of neurological deficit, larger infarct size, an increased tendency toward hemorrhagic transformation, a higher rate of early recurrent ischemic events, and elevated mortality. In populations with mixed etiological backgrounds, the proportion of cardioembolic mechanisms has been reported to be even higher [1,2,3]. In the Uzbek population, against the background of a high prevalence of atrial fibrillation, post-infarction myocardial remodeling, structural cardiac abnormalities, heart failure, cardiomyopathies, and valvular diseases, the true incidence of cardioembolic stroke has been increasing steadily in recent years. At the same time, population-specific and systematic data regarding the clinical course of this stroke subtype, inflammatory and biochemical parameters, biomarkers involved in thrombus formation, and genetic determinants in the local population remain limited and insufficiently investigated [4,5,6,7]. Although several important studies have addressed stroke epidemiology in Central Asian countries (Aringazina et al., 2018; Feigin, 2017), data on genetic profiles and the specific features of the cardioembolic stroke subtype remain scarce [8,9]. In particular, molecular genetic studies in the Uzbek population are extremely limited. Therefore, the present study is of substantial clinical and practical relevance.
2. Materials and Methods
- Study design and sample This study was designed to investigate the impact of MMP-9 and MMP-12 gene polymorphisms on stroke severity and was conducted as a single-center, regionally representative, prospective clinical and genetic study in a cohort of patients of Uzbek ethnicity admitted to the intensive neurology, intensive care (therapy and resuscitation), and neurology departments of the Tashkent State Medical University clinic. All patients were treated at the study clinical center during the predefined study period between 2024 and 2025. A total of 196 patients hospitalized with acute ischemic stroke were enrolled. According to the TOAST classification, 97 patients were classified as having cardioembolic stroke (CES) and 99 as having atherothrombotic stroke (ATS). The inclusion criteria were as follows: (1) age ≥18 years; (2) a confirmed diagnosis of ischemic stroke and its subtype based on instrumental investigations and established classification criteria; (3) Uzbek ethnicity and permanent residence in Tashkent city; and (4) provision of written informed consent by the patient or a legally authorized representative. A control group consisting of 30 individuals without a history of stroke or cardiovascular disease, matched for age and major clinical characteristics, was also recruited. The general clinical and demographic characteristics of the study population are presented in the table below.Laboratory methods The study was conducted in the laboratory of the higher education institution affiliated with Tashkent State Medical University. Written informed consent for genetic testing was obtained from all participants. Peripheral venous blood samples were used as biological material for molecular genetic analysis. Blood samples were collected during the acute or early subacute phase of stroke under sterile conditions into EDTA-treated vacuum tubes and processed under laboratory conditions for subsequent analyses. Genomic DNA was isolated using a spin-column (silica-based sorbent column) method in accordance with a standard extraction protocol. The quality and purity of the extracted DNA were assessed spectrophotometrically by evaluating the A260/A280 ratio. Polymorphisms in the promoter regions of the matrix metalloproteinase family genes, namely MMP-9 −1562 C/T (rs3918242) and MMP-12 −82 A/G (rs2276109), were investigated. Genotyping was performed using real-time polymerase chain reaction (real-time PCR, qPCR). Allele-specific fluorescent probes were applied, and genotyping was carried out in real time. During amplification, fluorescence signal intensity was automatically recorded at each cycle, and the cycle threshold (Ct) value was determined for each sample. Statistical analysesAnalysis was performed using IBM SPSS Statistics software (version 26.0). Quantitative variables with a normal distribution are presented as mean ± standard deviation (M ± SD), whereas non-normally distributed variables are expressed as median and interquartile range (Me [Q1; Q3]). Comparisons between two independent groups were conducted using Student’s t-test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables. In the molecular genetic analysis, genotype distributions were evaluated for conformity with Hardy–Weinberg equilibrium using the χ² test. Genotype and allele frequencies are presented as absolute numbers and percentages. Associations between clinical and genetic factors and clinical outcomes were assessed by calculating odds ratios (ORs) with 95% confidence intervals (95% CIs). To identify independent predictors of unfavorable clinical outcomes, multivariable logistic regression analysis was performed and their diagnostic performance was evaluated using receiver operating characteristic (ROC) curve analysis, including calculation of the area under the curve (AUC). All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
3. Results
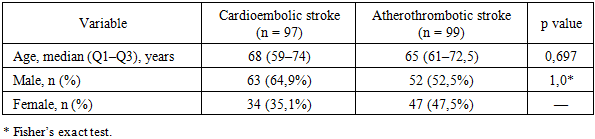
- Based on the comparison between the main and reference groups, the principal clinical and demographic characteristics of the patients were analyzed. According to the results, no statistically significant difference in median age was observed between the groups: the median age was 65 years (Q1–Q3: 61–72.5) in the atherothrombotic stroke group and 68 years (Q1–Q3: 59–74) in the cardioembolic stroke group (p = 0.697). Sex distribution analysis showed that males predominated in both groups, accounting for 52.5% of patients in the atherothrombotic stroke group and 64.9% in the cardioembolic stroke group. The proportion of females was 47.5% and 35.1%, respectively. According to Fisher’s exact test, no statistically significant difference in sex distribution between the groups was observed (p = 1.0).
|
|
|
|
4. Discussion
- When the results of studies reported in the international literature were compared, the role of inflammatory and genetic factors in both diagnosis and prognosis became clearly evident in cardioembolic stroke as well as in other stroke subtypes [10]. Another international study demonstrated that higher levels of the SII and NLR indices were associated with poor functional outcome after stroke and an increased risk of mortality, confirming the substantial impact of the inflammatory response on clinical outcomes [11]. Numerous studies and meta-analyses conducted in East Asian populations, particularly in China (Han), Korea, and Japan, have shown that the MMP-9 rs3918242 (−1562 C>T) polymorphism is associated with an increased risk of ischemic stroke and, in some cases, with hemorrhagic transformation [12]. In these populations, the T allele and the TT and CT genotypes have been considered risk-increasing factors for stroke, indicating the presence of ethnic differences in genetic susceptibility to the disease. In recent years, growing evidence has suggested that the MMP-12 gene plays a central role in the pathogenesis of stroke. In a study conducted in North Africa, particularly in the Tunisian population, an association was identified between the MMP-12 rs2276109 (−82 A>G) polymorphism and the risk of ischemic stroke as well as cardiovascular complications [13]. Importantly, the clinical relevance of this genetic variant was reported to be more pronounced when evaluated in the presence of diabetes mellitus. Thus, as shown by the analysis of the international literature, MMP-9 rs3918242 appears to be mainly relevant in East Asian populations, whereas MMP-12 rs2276109 shows notable associations in North African and some Asian populations [14,15]. The results obtained in the Central Asian population complement these regional findings by confirming the prognostic role of MMP-12 in a new ethnic context and by demonstrating the advantage of a comprehensive genetic assessment using the genetic burden score (GBS).
5. Conclusions
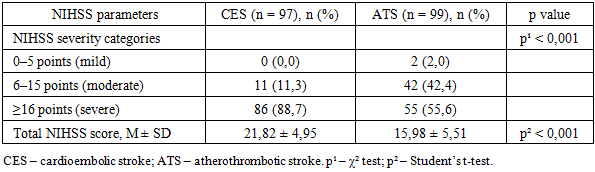
- According to the study results, in the investigated population, cardioembolic stroke was characterized by a more severe clinical course, a severe level according to the NIHSS (≥24 points) was observed significantly more frequently, and the degree of neurological deficit and functional limitation remained consistently high, as assessed by the NIHSS and modified Rankin scales. The high discriminative ability of the NIHSS score on day 1 for predicting a lethal outcome indicating the formation of a distinct “severe clinical phenotype” of cardioembolic stroke. A significant association between the MMP-12 rs2276109 (−82A/G) polymorphism and CEI, especially carriers of the A allele had approximately a two-fold higher risk of developing cardioembolic stroke. In univariate analysis, the AG and GG genotypes showed a protective effect with respect to lethal outcome, whereas the AA genotype was considered a high-risk variant. In contrast, the MMP-9 rs3918242 polymorphism did not demonstrate independent prognostic significance in the studied sample.