-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 842-845
doi:10.5923/j.ajmms.20261602.95
Received: Feb. 3, 2026; Accepted: Feb. 24, 2026; Published: Feb. 27, 2026

Clinical–Neurological and Motor Characteristics of Parkinson’s Disease: A Comparative Analysis of Disease Severity and Functional Impairment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSafarov Komiljon Kamolovich
PhD., Chief Doctor of the Bukhara District Medical Association, Bukhara, Uzbekistan
Correspondence to: Safarov Komiljon Kamolovich, PhD., Chief Doctor of the Bukhara District Medical Association, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor, cognitive, and neuropsychiatric impairments that significantly affect patients’ functional status and quality of life. Comprehensive clinical–neurological assessment remains essential for evaluating disease severity and identifying prognostic markers. A comparative clinical study was conducted involving patients with Parkinson’s disease divided into a main group and a comparison group, with an additional control group for selected parameters. Neurological, motor, cognitive, and psychoemotional status was assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS I–III), Hoehn and Yahr staging, Montreal Cognitive Assessment (MoCA), Beck Depression Inventory, olfactory testing, REM sleep behavior disorder assessment, and serum alpha-synuclein levels. Statistical analysis included Student’s t-test and Pearson’s χ² test.
Keywords: Parkinson’s disease, Motor dysfunction, UPDRS, Cognitive impairment, Alpha-synuclein, Clinical–neurological assessment
Cite this paper: Safarov Komiljon Kamolovich, Clinical–Neurological and Motor Characteristics of Parkinson’s Disease: A Comparative Analysis of Disease Severity and Functional Impairment, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 842-845. doi: 10.5923/j.ajmms.20261602.95.
Article Outline
1. Introduction
- Parkinson’s disease (PD) is a chronic, progressive neurodegenerative disorder characterized by a wide spectrum of motor and non-motor manifestations resulting from the degeneration of dopaminergic neurons in the substantia nigra pars compacta. The disease affects approximately 1–2% of the population over 60 years of age and represents one of the leading causes of neurological disability worldwide [1,2]. Despite significant advances in understanding the molecular and cellular mechanisms of PD, its clinical course remains heterogeneous, posing challenges for diagnosis, prognosis, and therapeutic decision-making. Traditionally, Parkinson’s disease has been defined primarily by its motor symptoms, including bradykinesia, rigidity, resting tremor, and postural instability. However, growing evidence indicates that non-motor manifestations, such as cognitive impairment, depressive disorders, sleep disturbances, autonomic dysfunction, and sensory abnormalities are integral components of the disease and may precede motor symptoms by several years [3,9,10]. These non-motor features substantially contribute to functional disability and reduced quality of life, often exerting a greater impact than motor impairment alone. Comprehensive clinical–neurological assessment using validated scales remains a cornerstone in the evaluation of Parkinson’s disease severity and progression. The Unified Parkinson’s Disease Rating Scale (UPDRS) provides a multidimensional assessment of cognitive, daily functional, and motor domains [3], while the Hoehn and Yahr scale is widely used to stage disease severity [4]. Cognitive screening tools such as the Montreal Cognitive Assessment (MoCA) and psychoemotional evaluations, including the Beck Depression Inventory, allow for early identification of non-motor dysfunctions that may influence treatment outcomes and disease prognosis. This article examines the mechanisms, diagnostic approaches, prognostic factors, and therapeutic strategies related to nephrotoxicity in metastatic breast cancer [5,6]. Special attention is given to the integration of prognostic markers and personalized medicine approaches aimed at improving renal outcomes while maintaining effective oncological treatment.In recent years, increasing attention has been directed toward the role of biomarkers and neurophysiological indicators in Parkinson’s disease. Alpha-synuclein, a key protein involved in the pathogenesis of PD, has been extensively studied as a potential biomarker reflecting neurodegenerative processes. In parallel, disturbances such as olfactory dysfunction and REM sleep behavior disorder have emerged as clinically relevant markers associated with disease progression and neurodegeneration [7].
2. Materials and Methods of Research
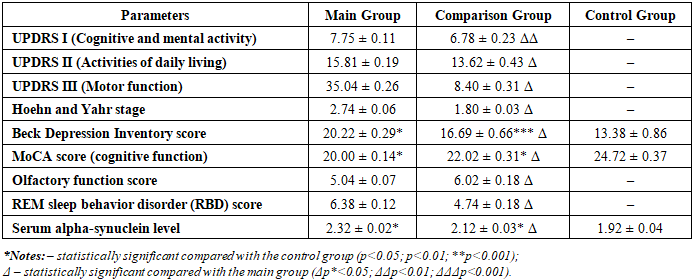
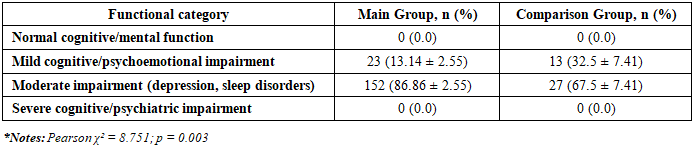
- A comparative clinical study was conducted involving patients diagnosed with Parkinson’s disease who underwent comprehensive clinical–neurological evaluation prior to treatment initiation. Patients were divided into two study groups: a main group and a comparison group. In addition, a control group of neurologically healthy individuals was included for selected non-motor and biomarker parameters. All participants provided informed consent prior to inclusion in the study, and the investigation was performed in accordance with the principles of the Declaration of Helsinki. Baseline clinical and neurological status was assessed using standardized and validated scales reflecting cognitive, functional, motor, and psychoemotional domains. Cognitive and mental activity was evaluated using Part I of the Unified Parkinson’s Disease Rating Scale (UPDRS I), while activities of daily living were assessed using UPDRS II. Motor function severity was determined using UPDRS III. Disease stage was classified according to the Hoehn and Yahr scale [4]. Depressive symptoms were assessed using the Beck Depression Inventory, and cognitive performance was evaluated with the Montreal Cognitive Assessment (MoCA) [7]. Additional non-motor parameters included olfactory function testing and evaluation of REM sleep behavior disorder symptoms. Serum alpha-synuclein levels were measured as a biochemical marker associated with neurodegenerative processes.The mean values of UPDRS I–III, Hoehn and Yahr stage, Beck Depression Inventory scores, MoCA scores, olfactory function indices, REM sleep disturbance scores, and alpha-synuclein concentrations were calculated and compared between the main, comparison, and control groups. These data constitute the basis of Table 1, which summarizes the clinical–neurological characteristics of the study groups prior to treatment.To further characterize disease severity, patients in the main and comparison groups were stratified according to functional impairment levels based on UPDRS I–III scores. For UPDRS I, patients were categorized into mild or moderate cognitive and psychoemotional impairment. For UPDRS II, levels of daily activity limitation were classified as moderate, severe, or associated with loss of independence. For UPDRS III, motor impairment was stratified into moderate, severe, and pronounced motor dysfunction with significant limitation of independent movement.The distribution of patients across these functional categories was analyzed using absolute values and percentage frequencies. Comparative analysis between groups was performed to identify differences in cognitive, daily functional, and motor impairment severity. These stratified functional outcomes are presented in Table 2, which provides a comparative analysis of functional status levels in the study groups before treatment.Statistical processing was performed using standard statistical software packages. Quantitative variables were expressed as mean ± standard error of the mean (M±m). Group comparisons of continuous variables were conducted using Student’s t-test. Categorical variables and frequency distributions were analyzed using Pearson’s χ² test. Differences were considered statistically significant at p < 0.05.
3. Results and Discussion
- Baseline clinical–neurological assessment revealed significant differences between the main and comparison groups prior to treatment initiation. Analysis of UPDRS Part I scores demonstrated a higher degree of cognitive and psychoemotional impairment in the main group, indicating more pronounced disturbances in mental and emotional functioning. In contrast, patients in the comparison group exhibited significantly lower UPDRS I scores, suggesting relatively preserved cognitive and affective status [4,9]. These findings underscore the heterogeneity of non-motor manifestations in Parkinson’s disease and support previous observations that cognitive and emotional dysfunction often parallels disease severity.Evaluation of daily living activities using UPDRS Part II showed significantly greater functional limitation in the main group compared with the comparison group. Patients in the main group demonstrated marked restrictions in everyday activities, whereas those in the comparison group retained higher levels of independence. Functional stratification based on UPDRS II revealed that severe limitations and loss of autonomy were predominantly observed in the main group, while moderate impairment was more characteristic of the comparison group. These results highlight the progressive impact of Parkinson’s disease on functional capacity and daily performance. Prior to treatment initiation, a comprehensive clinical–neurological evaluation was performed to assess baseline cognitive, functional, motor, and non-motor characteristics of patients with Parkinson’s disease. Standardized rating scales and laboratory markers were used to obtain an objective and multidimensional assessment of disease severity across the study groups. Comparative analysis focused on mental status, activities of daily living, motor impairment, psychoemotional condition, sleep disturbances, olfactory function, and serum alpha-synuclein levels. The summarized baseline clinical and neurological characteristics of the main, comparison, and control groups are presented in Table 1.
|
|
4. Conclusions
- The present study demonstrates significant clinical–neurological heterogeneity in patients with Parkinson’s disease at baseline, as evidenced by marked differences in cognitive, functional, motor, and psychoemotional parameters between the study groups. Patients in the main group exhibited more advanced disease stages, greater motor impairment, and more pronounced limitations in daily activities, as well as a higher burden of non-motor symptoms, including cognitive decline, depressive manifestations, sleep disturbances, and olfactory dysfunction. Functional stratification based on UPDRS I–III scores proved to be an effective approach for identifying clinically meaningful differences in disease severity. Higher UPDRS and Hoehn and Yahr scores were consistently associated with reduced independence, impaired cognitive performance, and increased motor disability. These findings confirm the multidimensional nature of Parkinson’s disease and emphasize the importance of comprehensive assessment beyond motor symptom evaluation alone. Elevated serum alpha-synuclein levels observed in patients with more severe clinical manifestations further support the role of this biomarker in reflecting neurodegenerative processes and disease progression. Integration of clinical scales with biochemical markers may enhance diagnostic accuracy and improve prognostic assessment.Overall, the results highlight the necessity of individualized evaluation and treatment planning in Parkinson’s disease. Comprehensive clinical–neurological assessment, incorporating motor and non-motor features as well as functional stratification, provides a robust foundation for optimizing therapeutic strategies and improving patient outcomes. Future studies should focus on longitudinal evaluation of these parameters to better define disease trajectories and refine personalized management approaches.