-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 834-836
doi:10.5923/j.ajmms.20261602.93
Received: Jan. 22, 2026; Accepted: Feb. 19, 2026; Published: Feb. 27, 2026

Risk Factors for Repeated Growth of Body Weight in Bariatric Patients and Optimization of Surgical Tactics
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBotirov J. A.1, Xayrullayev M. A.2, Botirov A. K.3, Otaqoziyev A. Z.4
1Doctor of Medical Sciences, Associate Professor, Department of Surgical Diseases, Andijan State Medical Institute, Andijan, Uzbekistan
2Free Applicant for the Department of Surgery Diseases, Andijan State Medical Institute, Andijan, Uzbekistan
3Doctor of Medical Sciences, Professor, Head of the Department of Surgical Diseases, Andijan State Medical Institute, Andijan, Uzbekistan
4Doctor of Philosophy, Associate Professor, Department of Surgical Diseases, Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The authors note that the conducted clinical and statistical analysis showed that the frequency of premature rupture of membranes in patients after RMPT is directly related to a number of key factors: the initial degree of obesity, body mass index, age, surgical method, and the diameter of the gastric tube used. The authors conclude that the use of optimized treatment-diagnostic and surgical tactics made it possible to significantly reduce the frequency of RMPT after RMPT by 19.1%. The algorithmized approach ensured a decrease in the frequency of repeated operations by 16.6% and a decrease in the frequency of immediate postoperative complications by 10.8%, which confirms its clinical advantage compared to traditional tactics.
Keywords: Obesity, Bariatric surgical interventions (BSI), RMPT - repeated gain of body weight, Type 2 diabetes mellitus is type 2
Cite this paper: Botirov J. A., Xayrullayev M. A., Botirov A. K., Otaqoziyev A. Z., Risk Factors for Repeated Growth of Body Weight in Bariatric Patients and Optimization of Surgical Tactics, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 834-836. doi: 10.5923/j.ajmms.20261602.93.
Article Outline
1. Introduction
- Repeated body mass gain (BMI) after bariatric surgeries remains one of the leading causes of a decrease in the long-term surgical effectiveness of obesity and associated metabolic disorders, as confirmed by data from modern domestic and foreign studies [2,3,5,6]. The lack of a unified approach to assessing the risk factors for repeated gain of body weight and choosing the optimal surgical tactics necessitates the variability of clinical outcomes and the increase in the number of repeated interventions [1,4].Purpose of the research. Algorithmized approach to preventing repeated weight gain after bariatric surgeries.
2. Research Material and Methods
- The study is based on a retrospective analysis of the results of surgical treatment of 1457 patients with obesity who underwent bariatric surgery in the period 2022-2025 at specialized surgical centers.Depending on the treatment-diagnostic and surgical tactics used, all patients were divided into two groups:- comparison group - 710 patients who used the traditional approach without differentiating the risk of repeated gain of body weight;- the main group consisted of 747 patients, whose treatment was carried out using optimized tactics based on algorithms for assessing risk factors and individualizing surgical parameters.The study included patients with morbid and high-degree obesity, including in combination with type 2 diabetes mellitus (type 2 DM). Exclusion criteria were repeated bariatric surgeries in the medical history, pronounced mental disorders, and non-compliance with recommendations in the early postoperative period.All patients underwent standard bariatric interventions, including longitudinal gastric resection and single-anastomous gastric bypass grafting. In the main group, the surgical parameters (calibration probe diameter, alimentary loop length) were selected individually, taking into account the initial degree of obesity, the presence of metabolic disorders, and the suspected risk of repeated weight gain.Repeated body mass gain was assessed based on the dynamics of body weight and body mass index in long-term observations. RMPT was understood as a clinically significant increase in body weight after reaching the minimum post-operative weight. An assessment of the risk factors for RMPT, the frequency of repeated surgical interventions, the structure and frequency of immediate postoperative complications, as well as the effectiveness of conservative treatment, was conducted.During examination, diagnosis, preoperative preparation, selection of bariatric surgical intervention methods, and postoperative management of patients with Graves' disease, it was carried out according to the generally recognized latest clinical recommendations, which were adopted and approved by the Ministry of Health of our Republic. Statistical processing of data was carried out using standard descriptive statistics methods. Quantitative indicators are presented as absolute values and percentages.
3. Results and Their Discussion
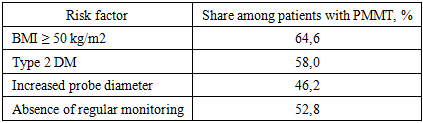
- RMPT was detected in 305 out of 1457 patients (21.0%). At the same time, the frequency of RMPT significantly differed between the studied groups (Table 1).
|

|
|
|

|
4. Conclusions
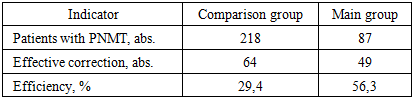
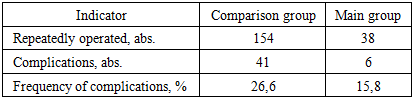
- Thus, the use of optimized therapeutic, diagnostic, and surgical tactics made it possible to significantly reduce the frequency of PMMT after BOD from 30.7% to 11.6% (a decrease of 19.1%). The algorithmized approach ensured a decrease in the frequency of repeated operations from 21.7% to 5.1% (16.6% decrease) and a decrease in the frequency of immediate postoperative complications from 26.6% to 15.8% (10.8% decrease), which confirms its clinical advantage compared to traditional tactics.