-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 811-816
doi:10.5923/j.ajmms.20261602.88
Received: Jan. 25, 2026; Accepted: Feb. 20, 2026; Published: Feb. 27, 2026

Perforations and Other Injuries of the Duodenum: Current Approaches to Diagnosis and Therapy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUrokov Sh. T.1, Abidov U. O.1, Masharipov Kh. K.2
1Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
2Bukhara Branch of the Republican Scientific Center for Emergency Medical Care Uzbekistan, Bukhara, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This review presents current aspects of diagnosis and treatment of peptic ulcer perforations and other duodenal integrity disorders, including retroperitoneal posterior wall injuries. It outlines etiological factors, classifications (including Stapfer), clinical features, imaging approaches, and treatment strategies. Special emphasis is placed on minimally invasive techniques - Over-the-Scope Clip (OTSC) and Endoscopic Vacuum Therapy (EVT) - which show high efficacy in selected cases and can reduce complication and mortality rates. The need for further research and broader implementation of these technologies in local clinical practice is highlighted.
Keywords: Ulcer perforation, Injury, Duodenum, Retroduodenal injury, OTSC, Endoscopic vacuum therapy
Cite this paper: Urokov Sh. T., Abidov U. O., Masharipov Kh. K., Perforations and Other Injuries of the Duodenum: Current Approaches to Diagnosis and Therapy, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 811-816. doi: 10.5923/j.ajmms.20261602.88.
1. Introduction
- This review presents up-to-date data on the diagnosis and treatment of peptic ulcer perforations and other conditions associated with disruption of the integrity of the duodenum (DU). Etiological factors, classifications of injuries, clinical manifestations, and diagnostic approaches are examined. Particular attention is paid to minimally invasive methods such as OVESCO (OTSC) placement and endoscopic vacuum therapy (EVT). The indications, technical aspects, and outcomes of these technologies are discussed both in comparison with and in combination with conventional surgery [3,4,5,8,15,19,20,21,22,23,24,25].Disruption of duodenal integrity is one of the key causes of emergency abdominal surgery and is associated with high mortality, especially in cases of delayed diagnosis and sepsis. Among the causes of duodenal wall disruption, perforations of ulcer etiology account for the majority, whereas trauma, anastomotic suture failure, and iatrogenic endoscopic injuries constitute the remaining proportion. Injuries of the posterior duodenal wall should be highlighted separately. With delayed diagnosis, mortality in these conditions may reach 40–70%, particularly with the development of peritonitis, retroperitoneal phlegmon, and sepsis [10,11,14].It is necessary to point out the existing challenges in early diagnosis and effective treatment of posterior duodenal wall injuries. The relevance and necessity of applying modern technologies in cases of posterior duodenal wall disruption are emphasized by a number of authors [1,2,7].The contemporary diagnostic and therapeutic approach relies on early imaging (primarily CT) and a personalized choice among surgical, endoscopic, and combined strategies. Major guidelines (WSES) emphasize the need for rapid stabilization, antibiotic therapy, and early source control, including laparoscopic repair or alternative methods in critically ill and high-risk patients [4,5,15].Disruption of the posterior wall of the duodenum represents a particularly rare and extremely serious pathology requiring immediate attention due to the high likelihood of complications and a significant risk of mortality. These injuries are often accompanied by atypical clinical presentations, which substantially complicates diagnosis. The main problem lies in the penetration of gastrointestinal contents into the retroperitoneal space, creating conditions for severe inflammatory processes such as phlegmon, abscess formation, and sepsis, as well as multiple organ failure [9,17,18].Diagnostics and Imaging. In cases of retroduodenal injuries, traditional examination methods such as diagnostic laparotomy and laparoscopy have limited effectiveness due to difficulties in accessing the retroperitoneal space, the inability to obtain sufficient diagnostic information, and the risk of developing various infectious complications.Therefore, this pathological condition requires the development of effective approaches aimed at reducing potential complications and improving treatment outcomes.There are also alternative approaches that lie between conservative and surgical management. These include stent placement, the use of biodegradable biological materials to close the defect at the site of injury, and the application of mesenchymal stem cells to accelerate healing processes. However, these methods are currently applied only at the experimental level and have not completed the full cycle of clinical trials; indications for their use, as well as their applicability across different patient populations, remain insufficiently defined [27].In some cases, conventional surgical techniques prove to be ineffective, which may necessitate repeated surgical interventions and, as a consequence, lead to increased mortality or reduced quality of life for patients.The diagnosis of retroduodenal perforations requires an integrated approach using modern imaging modalities. Contrast-enhanced computed tomography (CT) is considered the gold standard, as it allows detection of signs of perforation such as free gas or fluid in the retroperitoneal space.Contrast-enhanced CT is recommended as the method of choice for confirming perforation, localizing the defect, and assessing the extent of spread, including retroperitoneal involvement. Plain radiography for detection of “free gas” has low sensitivity; water-soluble contrast duodenography and/or duodenoscopy are used selectively, particularly when small or retroperitoneal defects or post-procedural complications are suspected.Magnetic resonance imaging (MRI) may be useful for detailed evaluation of soft tissues and assessment of the extent of the inflammatory process.Ultrasonography (US), especially when combined with Doppler imaging, helps identify fluid collections in the abdominal cavity, although it has limited diagnostic value for retroperitoneal processes.Laparoscopy serves as both a diagnostic and therapeutic modality, allowing visualization of the affected area and performance of necessary interventions.Clinical Presentation. Sudden onset of pain and signs of peritonitis are typical in cases of “free” perforation; in retroperitoneal rupture, the clinical picture is often more subtle and may include lumbar pain, subcutaneous emphysema, and fever.In recent years, an increase in the prevalence of chronic diseases has been observed. The growing number of patients with peptic ulcer disease, chronic inflammatory gastrointestinal disorders, and the use of gastrotoxic medications (e.g., NSAIDs, corticosteroids) contributes to an increased risk of perforation. In addition, patients with comorbid conditions such as diabetes mellitus, liver cirrhosis, and immunodeficiency states have a higher risk of complications.Atypical perforation, including retroperforation of a posterior duodenal wall ulcer, represents a rare but clinically significant problem that requires special attention in modern medicine. Its relevance is determined by several factors: high mortality rates, and the fact that delayed diagnosis and inadequate treatment lead to rapid progression of severe complications, including phlegmon, sepsis, and multiple organ failure. According to published data, mortality in advanced cases reaches 40–70%.Perforation of the posterior wall of the duodenum results in leakage of gastric contents rich in enzymes and acids into the retroperitoneal space. This triggers a rapidly progressing inflammatory process that may advance to retroperitoneal phlegmon, sepsis, and multiple organ failure.Diagnostic difficulties are primarily related to the atypical clinical presentation, which is associated with the confinement of gastrointestinal contents within the retroperitoneal space, hindering early detection. Standard diagnostic methods, such as plain radiography, are often of limited value, necessitating the use of advanced imaging techniques.The limitations of traditional treatment methods are related to the difficulty of accessing the retroperitoneal space and the high risk of infectious complications, which significantly complicate surgical management. This underscores the need to develop new, more effective, and safer therapeutic approaches.Thus, conditions associated with disruption of duodenal integrity—particularly perforations and injuries of the posterior wall of the duodenum—remain among the most complex and pressing problems in modern surgery, requiring innovative solutions and a multidisciplinary approach.Treatment. Alongside traditional conservative and surgical methods for managing conditions associated with disruption of duodenal integrity, modern minimally invasive technologies have been actively developed and introduced in recent years. These include endoscopic defect closure using OTSC systems, the use of endoscopic vacuum therapy (EVT) for anastomotic leakage and perforations, placement of temporary covered self-expanding stents, and the application of biodegradable materials for defect closure. These approaches make it possible to minimize surgical trauma, reduce the length of hospital stay, and lower the risk of postoperative complications. However, they require advanced technical resources and highly experienced specialists, and their effectiveness and indications within domestic healthcare settings have not yet been sufficiently studied [12,13].At the present stage, the treatment strategy for peptic ulcer perforations and disruptions of duodenal integrity is determined by the location of the defect, the time elapsed since injury, the severity of peritonitis, the patient’s general condition, and the technical capabilities of the healthcare facility.General principles of diagnosis and treatment have been developed in accordance with established guidelines (WSES, 2020; SAGES, 2019; ESGE, 2020). The core principles of management include immediate stabilization—correction of fluid and electrolyte disturbances and normalization of hemodynamics; broad-spectrum antibacterial therapy; antisecretory therapy; and early source control.Surgical Methods.1. Laparoscopic closure with Graham omentoplasty is considered the “gold standard” for small defects (<10–12 mm) in hemodynamically stable patients.2. Resection or duodenoplasty is indicated for larger defects.3. Retroduodenal injuries are surgically challenging due to limited access and often require a combined approach, including open surgical debridement and drainage of the retroperitoneal space.4. Endoscopic and minimally invasive technologies recommended by the ESGE (2020) include:- OTSC (OVESCO) is used for acute perforations up to 20 mm in size when detected early.- Endoscopic vacuum therapy (EVT) is indicated for anastomotic leaks, suture-line failure, and selected perforations; reported clinical success rates range from 80% to 100% in observational series.- Covered self-expanding stents are applied in cases of extended defects and when primary closure is not feasible.Table 1 summarizes the key approaches to the management of duodenal perforations, outlining their main indications, advantages, and limitations.
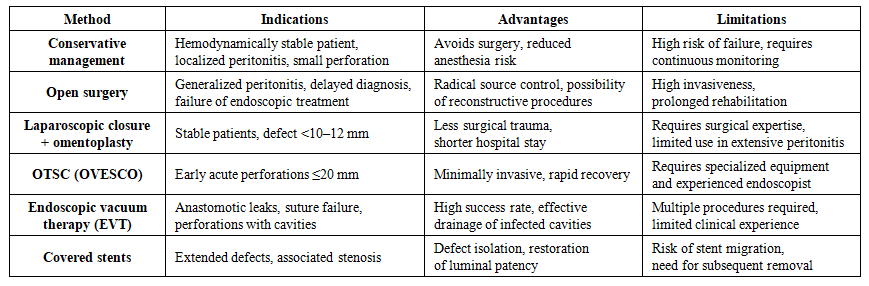 | Table 1. Comparative Characteristics of Treatment Methods for Duodenal Perforations |
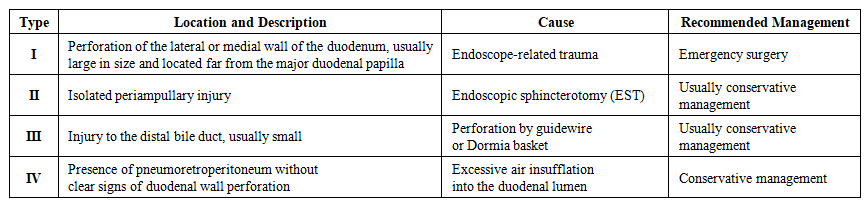 | Table 2. Classification of Iatrogenic Duodenal Injuries According to Stapfer and Recommended Management Strategy |
2. Conclusions
- Contemporary approaches to the diagnosis and management of duodenal perforations include early imaging (contrast-enhanced CT), adequate stabilization, and a targeted choice of treatment strategy based on the type of injury, defect size, and the patient’s clinical condition. Minimally invasive methods—OTSC and EVT—have demonstrated high clinical effectiveness, particularly in patients with high operative risk. Their wider implementation in clinical practice has the potential to reduce the number of re-laparotomies, shorten hospital stay, and decrease mortality rates.