-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 794-798
doi:10.5923/j.ajmms.20261602.84
Received: Jan. 28, 2026; Accepted: Feb. 20, 2026; Published: Feb. 27, 2026

Impact of Online Structured Education on Glycemic Control in Patients with Type 1 Diabetes Mellitus
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMahmudov Ulugbek Ilhomjon ogli1, Karimova Mukima Muhammadsadikovna2
1PhD Candidate, Department of Endocrinology, Phthisiology and Hematology, Fergana Medical Institute of Public Health, Uzbekistan
2PhD of the Department of Endocrinology, Phthisiology and Hematology, Fergana Medical Institute of Public Health, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Type 1 diabetes mellitus is a chronic autoimmune disease fully dependent on insulin, and its effective management largely depends on patients’ knowledge and self-monitoring skills. “Diabetes School” programs aim to improve glycemic control and prevent complications. This study evaluated the effectiveness of patient education using this program. The results demonstrated improved knowledge levels and better disease control indicators. Educational programs play an essential role in comprehensive diabetes management.
Keywords: Type 1 diabetes mellitus, Diabetes school, Patient education, Glycemic control, Self-monitoring
Cite this paper: Mahmudov Ulugbek Ilhomjon ogli, Karimova Mukima Muhammadsadikovna, Impact of Online Structured Education on Glycemic Control in Patients with Type 1 Diabetes Mellitus, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 794-798. doi: 10.5923/j.ajmms.20261602.84.
Article Outline
1. Introduction
- Type 1 diabetes mellitus (T1D) remains a serious global public health concern. In addition to its direct medical burden, it reduces quality of life, requires lifelong insulin therapy, and demands a high level of self-management skills. With the increasing prevalence of T1D, particularly among children and adolescents, the need for effective and accessible educational interventions is growing [1].The online format of a “Diabetes School” ensures broad access to information, enables repeated review of educational materials, supports interactive learning, and allows integration with modern glucose monitoring technologies. Contemporary systematic reviews demonstrate that diabetes self-management education and support (DSME/DSMES) programs improve HbA₁c levels, reduce the incidence of acute complications, and enhance self-management outcomes in patients with diabetes [4,7].The implementation and scientific evaluation of online “Diabetes School” programs in Uzbekistan have substantial practical significance for improving glycemic control, preventing complications, and strengthening evidence-based diabetes care.
2. Materials and Methods
- The study was conducted between 2023 and 2025 at the Fergana branch of the Republican Specialized Scientific and Practical Endocrinology Center. This tertiary referral center provides specialized endocrinological care and long-term follow-up for patients with diabetes mellitus, including pediatric, adolescent, and young adult populations.A total of 110 patients were enrolled in a prospective dynamic observation program. The inclusion criteria comprised: (1) laboratory-confirmed diagnosis of type 1 diabetes mellitus, (2) age between 9 and 30 years, and (3) disease duration ranging from 1 to 15 years. The mean age of participants was 16.8 ± 6.2 years, reflecting a predominantly adolescent cohort. Both male and female patients were included. Patients with severe concomitant chronic diseases or cognitive impairment that could limit participation in structured educational activities were excluded from the study.At baseline, all participants underwent a comprehensive clinical evaluation. Medical history was collected, including age at diagnosis, duration of diabetes, insulin therapy regimen (multiple daily injections or insulin pump therapy), frequency of self-monitoring of blood glucose, history of acute complications (hypoglycemia and diabetic ketoacidosis), and presence of chronic complications where applicable. Standard clinical and laboratory assessments were performed in accordance with national and international guidelines. These included measurement of glycated hemoglobin (HbA₁c), fasting and postprandial blood glucose levels, anthropometric parameters, and routine biochemical tests.The effectiveness of the educational intervention (“Diabetes School”) was assessed using a standardized questionnaire with a maximum score of 25 points. The questionnaire evaluated patients’ knowledge of key aspects of diabetes self-management, including insulin dose adjustment, carbohydrate counting, recognition and management of hypoglycemia and hyperglycemia, sick-day rules, dietary principles, and prevention of long-term complications. A score of ≥18 points was considered satisfactory, indicating an adequate level of theoretical knowledge and practical understanding necessary for effective self-management.Questionnaire-based assessment was conducted at three time points: prior to the initiation of the educational program (baseline), at 6 months, and at 12 months of follow-up. This longitudinal design allowed evaluation of both short-term and medium-term retention of knowledge and the sustainability of educational outcomes. Statistical analysis included comparison of baseline and follow-up results to determine the dynamics of knowledge improvement over time. Quantitative indicators were expressed as mean values with standard deviation (mean ± SD), and appropriate statistical tests were applied to assess the significance of observed changes.
3. Literature Review
- According to the International Diabetes Federation IDF Diabetes Atlas (11th edition, 2025), roughly 9.2 million people worldwide currently live with type 1 diabetes (T1D), including almost 1.8 million children and adolescents under 20 years of age [1]. These figures underline the substantial and growing global burden of T1D, which places long-term demands on patients, families, and health systems. T1D is associated with lifelong insulin dependence, frequent requirements for acute care for events such as severe hypoglycemia and diabetic ketoacidosis, and an elevated lifetime risk of microvascular and macrovascular complications that impair quality of life and increase mortality.Epidemiological modelling indicates that the true burden may be underestimated in routine reporting because of underdiagnosis, gaps in disease registries, and excess mortality in low- and middle-income settings. Data from modelling efforts and the T1D Index suggest that alternative assumptions about case ascertainment and survival produce substantially higher prevalence estimates; some models project total affected individuals approaching or exceeding 13 million under certain scenarios [2]. These modeling results highlight how surveillance limitations can mask the full public-health impact of T1D and reinforce the need for population-level strategies that include prevention of complications and strengthening of care delivery.The rising incidence of T1D—particularly among pediatric and adolescent age groups—creates important clinical, psychosocial, and economic challenges. Contemporary evidence emphasizes that effective diabetes management goes well beyond provision of insulin and routine clinical review: patient knowledge, practical self-management skills, psychosocial adaptation, family and community support, and access to diabetes technologies all substantially influence glycemic control, the frequency of acute and chronic complications, and overall wellbeing [3,10]. Several recent systematic reviews and meta-analyses concentrated on pediatric and adolescent populations demonstrate that structured educational and psychoeducational interventions are associated with clinically meaningful reductions in glycated hemoglobin (HbA₁c), fewer episodes of severe hypoglycemia and diabetic ketoacidosis, and measurable improvements in health-related quality of life and self-efficacy. For example, a comprehensive systematic review and meta-analysis published in Pediatric Diabetes synthesized controlled studies of educational interventions in young people with T1D and reported consistent benefits across multiple outcome domains [3,4].Structured “Diabetes School” programs—organized, curriculum-based DSME/DSMES interventions—are designed to deliver evidence-based instruction on pathophysiology, insulin management (including dose adjustment and carbohydrate counting), nutrition, physical activity, glucose monitoring (capable of integrating CGM data), sick-day management, and complication prevention. Participation in these programs increases disease-specific knowledge, strengthens practical self-management competencies, and frequently improves both clinical and psychosocial outcomes across diverse healthcare settings [5,6]. Importantly, group-based formats can provide peer support and normalize disease-related experiences, which may be especially beneficial for adolescents navigating developmental transitions.Digital and web-based DSME/DSMES interventions have expanded rapidly and are now supported by a growing body of evidence. Recent systematic reviews and meta-analyses of online diabetes education and digital health tools indicate that digital approaches can produce meaningful reductions in HbA₁c and improvements in self-management behaviors among children, adolescents, and adults with T1D. Digital platforms offer advantages such as asynchronous access, the capacity for repeated review of instructional content, interactive quizzes and decision aids, and the potential to integrate real-time glucose data from CGM systems—features that can enhance learning retention and support individualized problem solving [7,6]. These characteristics make online Diabetes School formats particularly attractive for regions with limited access to centralized face-to-face programs.Economic evaluations further support broader implementation of structured DSME/DSMES. Recent population-level analyses and cohort studies, including work published in BMC Health Services Research, report that participation in DSME programs is associated with reductions in total medical and prescription costs—often driven by fewer acute care visits, emergency department presentations, and hospitalizations. Reported reductions in adjusted total medical costs in some studies are on the order of 12–16%, and other analyses estimate per-patient annual savings in the range cited by public health agencies; these findings underscore the potential cost-effectiveness of investing in education as part of comprehensive diabetes care [8,9]. In addition to direct cost savings, improved self-management may yield broader economic benefits through reduced caregiver burden and improved school or work participation among patients.Taken together, these data justify the current study’s focus on evaluating a structured “Diabetes School” program. The primary aims are to assess changes in patient knowledge, self-management competencies, and glycemic outcomes following participation. The investigation is especially pertinent for contexts such as the Republic of Uzbekistan, where rising diabetes prevalence and limitations in organized patient education systems create an urgent need for scalable, effective interventions. Implementing and rigorously evaluating both face-to-face and online Diabetes School formats could inform national strategies to improve clinical outcomes, enhance patient empowerment, and optimize resource use within the healthcare system [8,9,10].
4. Clinical and Laboratory Results
- Among the patients included in the study, 52 individuals (47%) were boys and 58 (53%) were girls (Fig. 1). The mean age of the patients was 16.8 ± 6.2 years (median — 17 years; minimum age — 9 years; maximum — 25 years) (Fig. 1). The mean duration of the disease was 6.8 ± 3.2 years.The mean age of participants in Group 1 (offline training, n = 50) was 15.1 ± 3.4 years (range: 9 to 30 years). The mean duration of the disease was 6.7 ± 3.1 years; in 60% of patients (30 individuals), the disease duration did not exceed 5 years, whereas in 40% (20 individuals) it was more than 5 years.The mean age of participants in Group 2 (online training, n = 60) was 15.4 ± 3.6 years (range: 9 to 30 years). The proportion of urban residents was 48% (29 individuals), while 52% (31 individuals) were from rural areas. The mean duration of the disease was 6.9 ± 3.3 years; in 63% of patients (38 individuals), the duration did not exceed 5 years, whereas in 37% (22 individuals) it was more than 5 years.At the initial stage of observation, carbohydrate metabolism parameters in both groups were comparable. No statistically significant differences were found in baseline glycated hemoglobin (HbA1c) levels (p > 0.05). These findings indicate that the groups were comparable in terms of type 1 diabetes compensation at the start of the study.Upon completion of the educational cycle, that is, after 6 months, positive changes in carbohydrate metabolism parameters were observed in both groups. However, the magnitude and statistical significance of these changes differed between the groups.In the control group that underwent face-to-face training, the HbA1c level decreased from 9.0% [8.1–10.0] to 8.2% [7.8–8.9]. In contrast, the online training group demonstrated a more pronounced and statistically significant reduction in HbA1c levels — from 8.7% [7.6–9.5] to 7.5% [6.6–7.9] (p < 0.001) (Fig. 1).
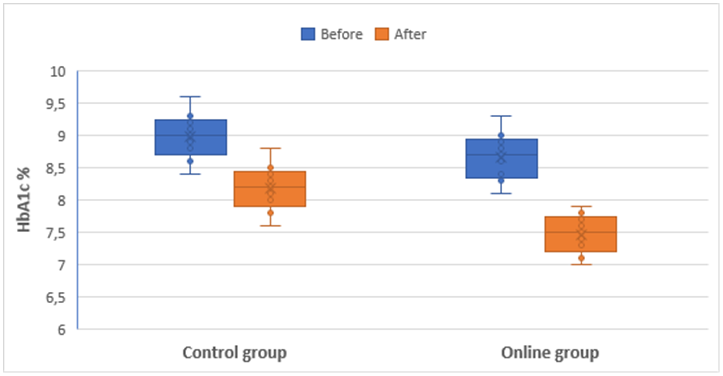 | Figure 1. Dynamics of HbA1c levels in the control and online groups before and after the educational intervention |
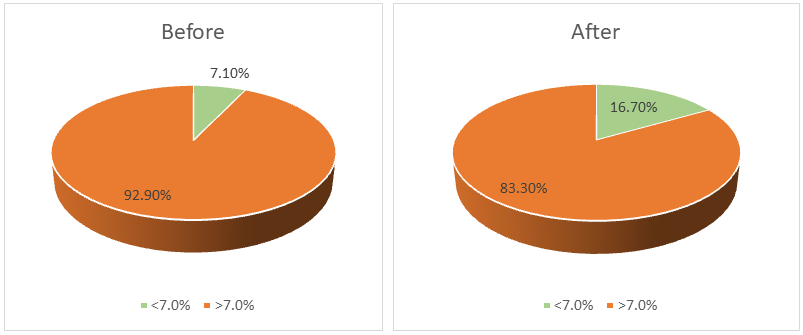 | Figure 2. Proportion of patients in the control group who achieved the target HbA1c level before and after the educational intervention |
5. Conclusions
- The results of the study demonstrated that the “Diabetes School” program significantly improves patients’ awareness of their disease and facilitates the development of effective self-management skills. This, in turn, contributes to a reduction in the frequency of acute complications of diabetes mellitus, including diabetic ketoacidosis and severe hypoglycemia. Although the follow-up period was relatively limited, the statistically significant decrease in glycated hemoglobin (HbA1c) levels may be considered a prognostic indicator of a reduced risk of chronic complications, as improved glycemic control is directly associated with their prevention and delayed progression.Comparative analysis showed that both online and traditional face-to-face educational formats positively influence self-management competencies and glycemic outcomes. However, the дистанционный (remote) learning format demonstrated greater effectiveness, likely due to the flexibility of accessing materials at a convenient time, the possibility of repeated review of educational sessions, and the use of interactive teaching methods that enhance engagement and knowledge retention.It was also established that participation in the “Diabetes School” program increases adherence to insulin therapy, promotes compliance with principles of balanced nutrition, encourages regular self-monitoring of blood glucose, and supports timely prevention of complications. In addition, the program exerts a positive impact on patients’ psychological well-being, strengthens motivation for long-term disease control, and fosters a responsible attitude toward personal health.Overall, the “Diabetes School” program represents an effective tool for comprehensive management of type 1 diabetes mellitus. Its broader implementation within the healthcare system may contribute to improved quality of life, reduced risk of both acute and chronic complications, and optimization of healthcare expenditures through better long-term disease control.