-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 774-779
doi:10.5923/j.ajmms.20261602.80
Received: Feb. 3, 2026; Accepted: Feb. 23, 2026; Published: Feb. 27, 2026

Cognitive Disorders in Post-Traumatic Encephalopathies and Increase the Effectiveness of Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHikmatova Sh. Sh., Haydarov N. Q., Abdullaeva M. B., Sobirova S. K., Aduqodirov E. I.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Post-traumatic encephalopathy (PTE) is a chronic progressive condition that develops after traumatic brain injury and is characterized by cognitive, morphological, and functional impairments of the central nervous system. The present study aimed to evaluate cognitive disorders in patients with PTE and assess the effectiveness of комплекс therapy. A total of 100 patients were examined using clinical, neuropsychological (MMSE), neuroimaging (MRI), and functional (EEG) methods before and after treatment. Prior to therapy, most patients demonstrated pre-dementia cognitive impairment (MMSE 24–25 points), along with diffuse cerebral atrophy, gliosis, leukoaraiosis, and pathological EEG changes. After комплекс treatment, MMSE scores improved to 26–27 points, accompanied by stabilization of MRI findings and normalization of EEG parameters. The results confirm the interrelationship between structural, functional, and cognitive disturbances in PTE and demonstrate the clinical effectiveness of timely comprehensive therapeutic intervention.
Keywords: Post-traumatic encephalopathy, Traumatic brain injury, Cognitive impairment, MMSE, MRI, EEG, Neurodegeneration, Комплекс therapy, Cerebral atrophy
Cite this paper: Hikmatova Sh. Sh., Haydarov N. Q., Abdullaeva M. B., Sobirova S. K., Aduqodirov E. I., Cognitive Disorders in Post-Traumatic Encephalopathies and Increase the Effectiveness of Treatment, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 774-779. doi: 10.5923/j.ajmms.20261602.80.
1. Introduction
- Encephalopathy is a brain injury that leads to degeneration of nerve tissue and is characterized by impaired cerebral function. [1] Pathological impairment of cerebral function occurs mainly through two mechanisms:Ischemia occurs as a result of insufficient oxygen reaching the cells of the brain due to damage to the blood vessels of the brain. This can be caused by arterial hypertension, diabetes, atherosclerosis, thrombosis, etc. [2]Intoxication is poisoning by products that are harmful for metabolism to brain cells. This condition often occurs as a result of long-term alcohol consumption, liver diseases, kidney diseases, etc. [3]Encephalopathy is most common in people over 50 years of age. However, the disease is now becoming more common in younger people. It can even occur in newborns (perinatal encephalopathy), caused by hypoxia during pregnancy. [4]Another type of encephalopathy that is currently becoming increasingly serious and has serious consequences is post-traumatic encephalopathy. Post-traumatic encephalopathy (PTE) is a group of mental and neurological disorders that include atrophic, dystrophic, and degenerative changes in the layers of the brain that develop over one or more years after a traumatic brain injury. [5] The symptoms and degree of damage to the PTE depend on the patient's age, the severity of the traumatic brain injury, the effect of medical treatment, changes in the blood vessels of the brain, and the effects of chronic and alcoholic intoxication. [10-11]Symptoms of posttraumatic encephalopathy: memory loss, weakness, headache, dizziness, ringing in the ears, depressed mood, speech disorders, tremors, urinary disorders. [6,7]80% of injuries in neurotraumatology are mild traumatic brain injuries, which occur in an average of 120 to 300 people per 1,000,000 population in different countries. [12-14] In addition, due to modern urbanization and the increase in the number of vehicles on city roads, traumatic brain injuries, as well as post-traumatic encephalopathy, which occurs after injuries, are becoming the most urgent problem. [15] Complications arising from various traumatic brain injuries worsen the quality of life of patients and make their social adaptation difficult. [9] The fact that traumatic brain injuries are more common, especially in young people, causes many social problems. [14-16] Therefore, timely diagnosis of such patients and improvement of treatment tactics have become an urgent task.The purpose of the study: to evaluate the development of post-traumatic encephalopathies and to develop effective diagnostic and therapeutic measures.
2. Research Material and Methods
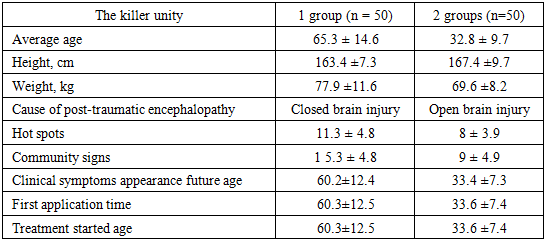
- 100 patients with post-traumatic encephalopathy participated in our clinical study, their average age was 23-80 years. The differences in age and gender of the patients are described in Table 1. All the patients included in our study were divided into two groups: 50 patients received conventional treatment and 50 patients received complex treatment.
|
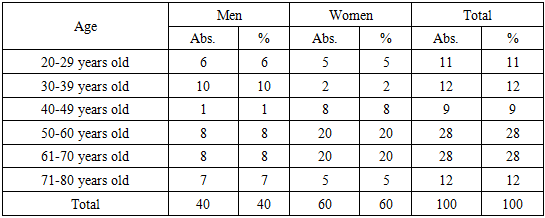
 | Figure 1. Average age of patients by gender |
|
3. Research Results
- The cognitive function of 100 patients with post-traumatic encephalopathy included in the study was assessed using the MMSE scale. According to the results, the majority of patients had MMSE scores in the range of 24–26.The most common MMSE scores during the follow-up period were 24 and 25 points, indicating that a large proportion of patients had predementia cognitive impairment. Although scores of up to 26 points were observed in some patients, results that fully corresponded to normal cognitive function (28–30 points) were almost nonexistent.MMSE scale to the interpretation suitable:• 24-27 points - preliminary cognitive disruptions,• 20-23 points - mild dementia,• 28-30 points - cognitive violations no.This from the criteria come out without, in the study participation did of patients in most cases cognitive violations clinical in terms of formed, however still dementia to the level insufficient situation that It was determined. This situation post-traumatic in encephalopathy cognitive functions decrease chronic and progressive to the feature owner that it is confirms.Also, the accumulation of MMSE scores in a relatively narrow range (mainly 24–25) indicates the presence of a uniform clinical profile of cognitive deficits, namely, moderate impairments in memory, attention, calculation, and executive functions predominate. According to the results of the analysis of 100 patients with post-traumatic encephalopathy, the majority of patients had MMSE scores in the range of 24–26 points, which indicates the predominance of pre-dementia cognitive impairment. The identified changes confirm the presence of a persistent decline in cognitive functions in post-traumatic encephalopathy and justify the need for early neuropsychological diagnosis, dynamic monitoring, and cognitive rehabilitation measures in these patients.After a course of treatment, cognitive function was reassessed in 100 patients with post-traumatic encephalopathy. The results showed that MMSE scores were mostly in the range of 25–27.The most common values after treatment were 26 and 27 points. This indicates a positive trend compared to the pre-treatment values of around 24–25 points. Although in some patients MMSE scores remained at 25 points, in most cases an improvement in cognitive functions was noted.MMSE scale to the interpretation suitable:• 28-30 points - cognitive violations no,• 24-27 points - preliminary cognitive disruptions,• 20-23 points - mild dementia.When analyzed based on these criteria, pre-dementia cognitive impairments remained in the majority of patients after treatment, but their severity significantly decreased. In particular, a steady trend of improvement was observed in the indicators of attention, short-term memory, calculation, and orientation functions.The shift of MMSE scores to the upper limit (26–27 points) indicates that the treatment measures have a positive effect on cognitive functions, and the neuropsychological deficit is reversible. This confirms the effectiveness of comprehensive and timely therapy in post-traumatic encephalopathy. The results of the assessment of 100 patients with post-traumatic encephalopathy after treatment showed an increase in MMSE scale indicators to the range of 25–27 points. This confirms that as a result of treatment, cognitive functions have significantly improved, the risk of dementia has decreased, and there is a possibility of functional recovery of cognitive disorders. The results obtained substantiate the important clinical significance of the MMSE scale in assessing the effectiveness of treatment in patients with post-traumatic encephalopathy.
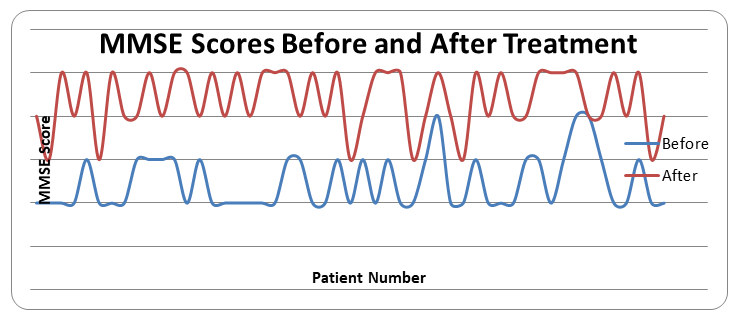 | Figure 2. MMSE scores before and after treatment |
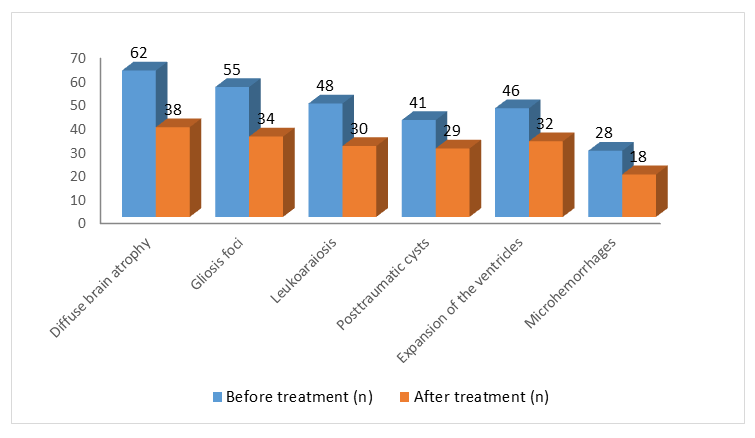 | Figure 3. MRI findings before and after treatment |
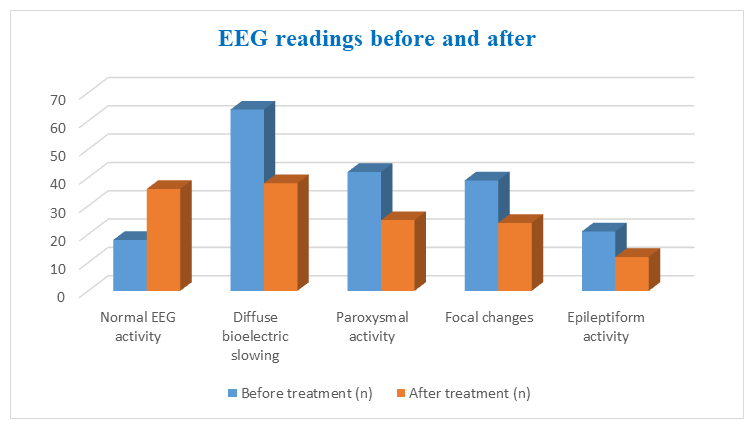 | Figure 4. EEG readings before and after treatment |
4. Conclusions
- The development of SBE in patients with SCD significantly worsens the quality of life of patients. Patients develop SBE, which causes complications in many other systems. Post-traumatic encephalopathy is also characterized by complications involving the nervous system, including the peripheral nervous system. Neurological dysfunctions observed in post-traumatic encephalopathy lead to a sharp decrease in the quality of life of patients.Seizure syndrome lasting more than three months, a significant increase in cerebral hypertension during physical activity was observed.Deep reflex assessment revealed asymmetric reduction of various reflexes, and in some patients complete loss of reflexes was observed. It is noteworthy that in a large proportion of patients, seizures and cognitive impairment were detected and corrected.Overall, these results highlight the complexity of neurologic manifestations and severe clinical manifestations in patients with posttraumatic encephalopathy, emphasizing the importance of comprehensive evaluation and management strategies to address cerebral complications in this patient population.