-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 771-773
doi:10.5923/j.ajmms.20261602.79
Received: Dec. 30, 2025; Accepted: Jan. 20, 2026; Published: Feb. 26, 2026

Methods of Surgical Correction of Mid-Shaft Hypospadias in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbonmurod Niyozovich Ibragimov1, Yusufjon Makhmudovich Akhmedov2, Islamjon Yusufjonovich Akhmedov3
1Regional Children's Multidisciplinary Medical Center, Samarkand, Uzbekistan
2Head of the Department of Pediatric Surgery No. 2, Samarkand State Medical University, Samarkand, Uzbekistan
3Assistant of the Department of Pediatric Surgery No. 2, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Hypospadias is a common genital anomaly. Treatment of hypospadias in children is performed only surgically. The variety of treatment methods used is due to the large number of interventions and the search for surgical methods to correct hypospadias.
Keywords: Hypospadias, Urethroplasty, Penile malformation, Pediatric urology, Genital reconstruction
Cite this paper: Kurbonmurod Niyozovich Ibragimov, Yusufjon Makhmudovich Akhmedov, Islamjon Yusufjonovich Akhmedov, Methods of Surgical Correction of Mid-Shaft Hypospadias in Children, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 771-773. doi: 10.5923/j.ajmms.20261602.79.
1. Introduction
- Hypospadias is one of the most common congenital anomalies of the male genital organs. Treatment of hypospadias in children is carried out surgically. The variety of treatment methods used is due to the high number of postoperative complications and the ongoing search for the optimal surgical approach for correcting hypospadias. More than 300 different surgical techniques for hypospadias correction have been proposed; however, the complication rate remains significant—ranging from 10% to 45%, depending on the type of deformity. [1]According to the World Health Organization (WHO), “congenital malformations affect one in every 33 newborns worldwide each year.” Among pediatric urological anomalies, the incidence of hypospadias has been steadily increasing (Springer A., van den Heijkant M., Baumann S., 2015). [2]According to the Barcat classification (1973), there are three main types of hypospadias:Anterior hypospadias, which includes glanular, coronal, and distal penile forms;Middle (midshaft) hypospadias;Posterior hypospadias, which includes proximal penile, penoscrotal, scrotal, and perineal forms.This study is devoted to analyzing the results of surgical treatment in patients with midshaft hypospadias, based on a sample of 179 patients aged 1 to 16 years.To date, more than 300 different surgical correction techniques have been developed for this anomaly. In our study, the following surgical methods were used for midshaft hypospadias correction: Mathieu, Duplay, and TIP (Tubularized Incised Plate). Despite the wide variety of surgical techniques available, none of them can be considered ideal. Further research is needed to determine the optimal age for surgery, indications for different surgical approaches, and best postoperative management techniques, including urinary drainage and wound care. [3]Objective of the StudyTo improve surgical outcomes in children with midshaft hypospadias by identifying factors influencing the rate of postoperative complications.
2. Materials and Methods
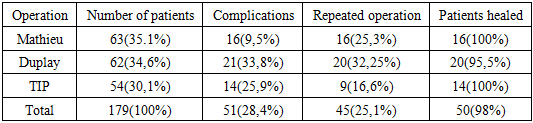
- From 2015 to 2023, in the Department of Pediatric Surgery of the Samarkand Regional Multidisciplinary Medical Center (RMMMC), 179 patients aged 1 to 16 years with midshaft hypospadias were examined and treated.All patients underwent comprehensive preoperative assessment and subsequent surgical correction. The diagnostic evaluation included:Medical history and physical examination;Ultrasound (US) of the pelvic organs;Cystoscopy;Genetic analysis;Standard laboratory tests.All patients underwent surgical treatment. During surgery, attention was given to the optimal method of urinary diversion, the use of modern suture materials, and appropriate postoperative care. [4]The following surgical techniques were used:Mathieu procedure – performed in 63 patients (35.1%); complications were observed in 16 patients (9.5%).TIP procedure (Snodgrass) – performed in 54 patients (30.1%); complications occurred in 14 patients (25.9%).Duplay procedure – performed in 62 patients (34.6%); complications were noted in 21 patients (33.8%). [5]These findings indicate that while all three methods are applicable, TIP and its modifications demonstrate higher efficiency and lower complication rates compared to the Duplay technique, making them more favorable for surgical correction of midshaft hypospadias in pediatric patients.
 | Figure 1. Stages of Surgery for Penile (Shaft) Form of Hypospadias |
3. Results and Discussion
- Thus, for mid-penile hypospadias, 179 children underwent surgical interventions using 3 methods. With the Mathieu method, complications were observed in 16 (9.5%) patients: 7 patients developed a postoperative urethral fistula, and 9 experienced urethral suture dehiscence. In patients with a fistula, closure using the Smith technique was performed 6 months after the initial surgery. Six children achieved a positive result after repeat surgery. The fistula recurred in one patient, which required its repeat closure by Smith. Of the 9 patients with urethral suture dehiscence, repeat intervention was performed in 8, while the parents of one patient refused further treatment. [6]For the Duplay operation, complications occurred in 21 (33.8%) patients. Of these, 14 developed a fistula, which required another operation (fistula closure by Smith) after 6 months. In 3 boys, dehiscence recurred in the postoperative period, and 6 months later, a Mathieu operation was performed with a positive surgical result of urethroplasty. One boy with a fistula was lost to follow-up, as he did not present for the scheduled repeat surgical treatment, and his further fate is unknown to us. Scar deformity was observed in 7 patients, which required repeat surgery. [7]For the TIP method, complications occurred in 14 (25.9%) patients: 9 boys developed a urethral fistula and 5 developed meatal stenosis. The fistula in 9 patients was closed by Smith 6 months after the operation. Patients with diagnosed meatal stenosis underwent meatoplasty with a positive result. (Table 1).
|
4. Conclusions
- Thus, the lack of a unified approach to treatment, the high incidence of postoperative complications, and the significant social relevance confirm that research devoted to the surgical treatment of hypospadias is both timely and justified. The TIP (Tubularized Incised Plate) operation and its author’s modification for proximal hypospadias demonstrate greater effectiveness and the lowest rate of complications compared to the Duplay procedure.The standardization of methodological approaches to the surgical treatment of various forms of hypospadias contributes to minimizing complications and shortening the urethral recovery period. [10]The success of hypospadias treatment in children depends not only on the correct choice of surgical technique but also equally on numerous aspects of postoperative management — including the optimal method of urinary diversion, proper dressing application, and the use of modern atraumatic suture materials and microsurgical instruments, all of which significantly improve the outcomes of surgical treatment for hypospadias.