-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 761-766
doi:10.5923/j.ajmms.20261602.77
Received: Jan. 18, 2026; Accepted: Feb. 15, 2026; Published: Feb. 26, 2026

Improving Treatment Adherence Among Patients Living in District Areas with Chronic Cardiovascular and Respiratory Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJ. A. Rizaev1, Sh. A. Khusinova1, A. G. Gadaev2
1Samarkand State Medical University, Samarkand, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article examines treatment adherence among the population living in district areas, using the example of the Samarkand region, focusing on patients with cardiovascular and respiratory diseases. Treatment adherence was assessed using the widely applied Morisky–Green questionnaire. The reasons for patients’ low adherence to treatment and non-compliance with medical recommendations are identified. These factors are directly related to patient-related issues as well as insufficient communication between physicians and patients. To accelerate the integration of modern technologies into practical healthcare in this field, an electronic application was developed and implemented in clinical practice.
Keywords: Arterial hypertension, Ischemic heart disease, Chronic heart failure, Bronchial asthma, Chronic obstructive pulmonary disease, Dorivaqti.uz
Cite this paper: J. A. Rizaev, Sh. A. Khusinova, A. G. Gadaev, Improving Treatment Adherence Among Patients Living in District Areas with Chronic Cardiovascular and Respiratory Diseases, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 761-766. doi: 10.5923/j.ajmms.20261602.77.
Article Outline
1. Introduction
- Experts of the World Health Organization (WHO) call the increase in the prevalence of chronic non-communicable diseases the epidemic of the 21st century [13]. Among them, diseases of the cardiovascular system and respiratory organs, including coronary heart disease, arterial hypertension, chronic heart failure, bronchial asthma, chronic obstructive pulmonary disease, occupy a leading position and in most cases lead to a sharp deterioration in the quality of life of patients, an increase in the number of re-hospitalizations, a sharp increase in the cost of treatment and death.Coronary heart disease is widespread in our Republic, as in European countries, and is a leading cause of death [12]. In most cases, arterial hypertension and coronary heart disease are ultimately complicated by chronic heart failure. The number of patients suffering from it, according to 2016 data, amounted to more than 26 million people worldwide [7]. The funds spent amounted to 2-3% of healthcare expenditures, and these figures are expected to double in the next 20 years [1]. As in the rest of the world, in our Republic, due to the increase in the number of elderly people, there is a possibility of a sharp increase in spending on them in the next 10 years [5]. According to 2016 data, more than 208 billion dollars were spent on the treatment of chronic heart failure by the global healthcare system. Chronic obstructive pulmonary disease is among the top ten causes of death in the world. In 2016, 251 million patients with this disease were registered worldwide [8]. This situation poses a major challenge to global medicine due to the high cost of treatment and the negative impact on patients' quality of life. In addition, chronic obstructive pulmonary disease is one of the leading causes of death. It has been shown that between 2009 and 2019, mortality from it increased by 35.4% [11]. According to experts from the World Health Organization, this disease is predicted to become the third leading cause of death by 2030 [9].Along with chronic obstructive pulmonary disease, bronchial asthma is a leading cause of death among respiratory diseases. According to data from 2019, this disease was diagnosed in 262 million people worldwide, and 455,000 of them died [4]. One of the reasons for the high incidence of adverse outcomes in patients is their low adherence to treatment, i.e., low compliance. Although a number of studies have been conducted in leading countries of the world on this issue, no studies have been conducted in Uzbekistan to study the adherence of patients to treatment for chronic diseases that are widespread among the population [13]. The importance of this problem was first announced by the World Health Organization in 2003, when it was shown that in developed countries, the average adherence of patients with chronic diseases to long-term treatment is 50%, and in developing countries it is even lower. In more recent studies, this figure has been reported to be 30–70% in patients with coronary heart disease [12]. These trends have been termed the “adherence pandemic” by Kolandanvelu et al. (2014).Non-adherence or inadequate adherence to medical advice is now a well-established risk factor for all diseases. It reduces the effectiveness of treatment, increases costs, increases the likelihood of various complications, and negatively affects disease outcome and life expectancy [2].Various methods have been proposed to determine adherence to treatment. Indirect methods include patient questionnaires, daily self-monitoring, counting the number of medications used or prescribed and dispensed, measuring various physiological markers, inserting electronic chips into the drug packaging, and using microsensors that activate in the stomach. Although the latter methods are objective, they are very expensive and therefore have limited applicability in daily practice [16].Currently, the Moriskey-Green, Moriskey Treatment Propensity Assessment, Martin-Bauarte-Green questionnaire, and others are used in practice. Each of them has its own advantages and disadvantages [15].Donald E. Moriskey and co-authors conducted logistic regression and found that several modified variables can predict treatment propensity. According to the results of the model, those who have knowledge about arterial hypertension, feel satisfied, and have skills to overcome difficulties are more likely to maintain treatment regimens [10].It is known that arterial hypertension, angina pectoris and related chronic heart failure, as well as respiratory diseases, including chronic obstructive pulmonary disease, bronchial asthma, are widespread pathological conditions throughout the world, including in our Republic. Unfortunately, the susceptibility of patients to treatment, the reasons leading to its low adherence, and the level of adherence to standard treatment methods proven to be effective in diseases recorded by primary care physicians have not been studied.Research objective: To study the treatment preferences of patients with chronic diseases that are widespread in primary health care institutions in the Pastarghom and Jamboy districts of the Samarkand region and to improve it using digitalization.
2. Materials and Methods
- Our study involved 1012 patients with hypertension (HG), coronary heart disease (CHD), chronic heart failure (CHF), bronchial asthma (BA) and chronic obstructive pulmonary disease (COPD) living in the Pastarghom and Jamboy districts of the Samarkand region. Information about them is presented in Table 1 below.
|

3. Research Results and Discussion
- As we noted above, the lack of full acceptance of generally accepted and recommended treatments for chronic diseases by patients, that is, low adherence to treatment or their non-prescription by doctors according to standards, is currently one of the important problems of medicine. Taking into account the great importance of the violation of all links in this chain, we comparatively studied the treatment preferences of patients living in the studied regions using the Moriski Green questionnaire.Based on the results of the Moriski Green survey, it is observed that the willingness to receive treatment in patients with cardiovascular and respiratory diseases in the district of Samarkand region is at an average and lower level. In order to change the willingness to receive treatment in a positive direction, a number of new methods are being recommended, combining the achievements of modern science in the world. In this area, extensive work is being carried out in our Republic on digitalization in all areas, including medicine. As we have emphasized above, we have created and implemented a mobile electronic program that provides for the interaction of doctors and patients, which helps to increase the willingness of patients to receive treatment. In the next stage of our monitoring, a re-survey was conducted among the population under our monitoring who were diagnosed with cardiovascular and respiratory diseases in the central family polyclinics of Pastargam and Jamboy districts of Samarkand region after the introduction of the electronic program, and the results are presented in Figure 1.
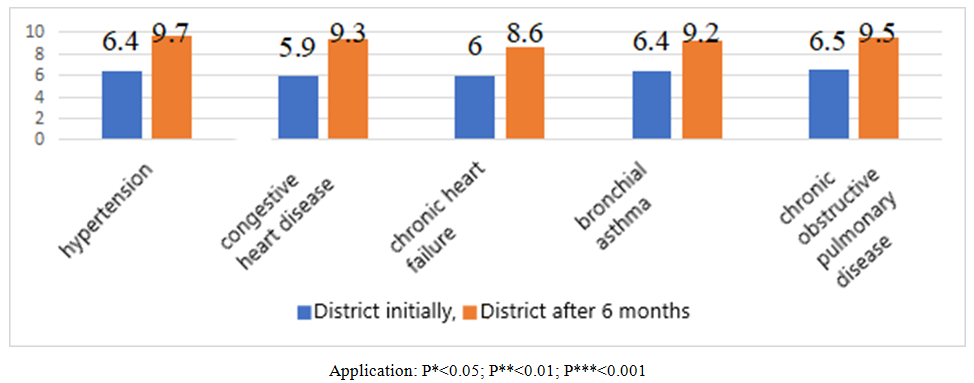 | Figure 1. Treatment propensity scores (scores) determined using the Moriski Green questionnaire before and after the introduction of the electronic program in patients living in the district center with cardiovascular and respiratory diseases |
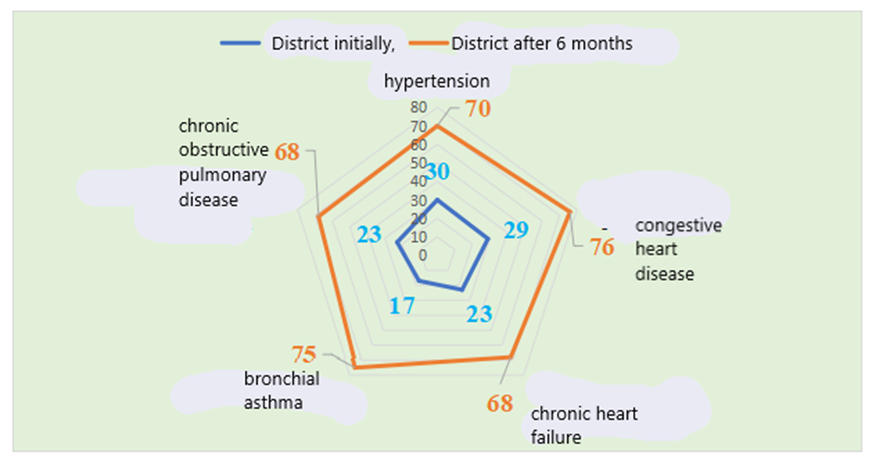 | Figure 2. High treatment adherence rates (in absolute numbers) determined using the Moriski Green questionnaire after the introduction of the electronic program in patients living in a district with cardiovascular and respiratory diseases |
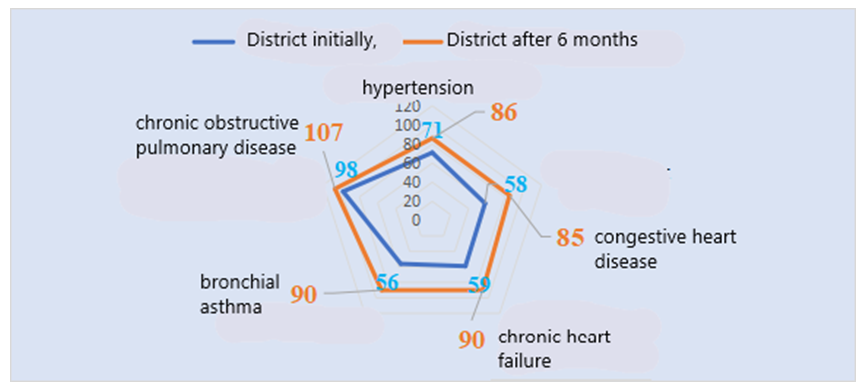 | Figure 3. Average treatment adherence rates (in absolute numbers) determined using the Moriski Green questionnaire after the introduction of the electronic program in patients living in a district with cardiovascular and respiratory diseases |
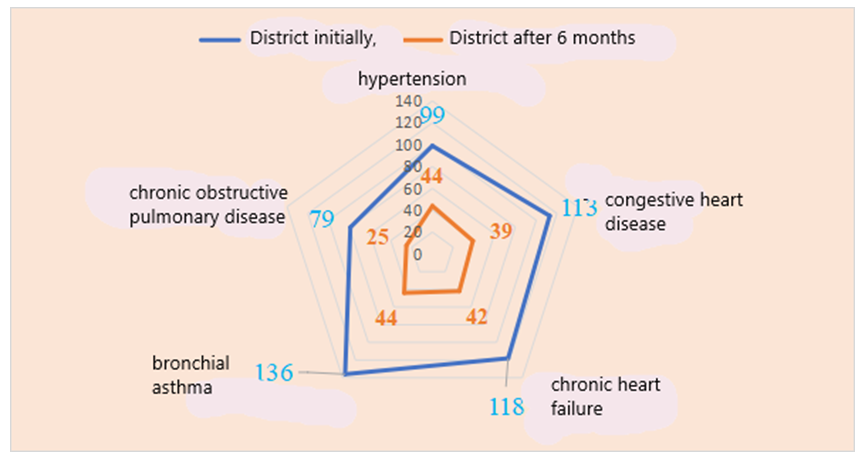 | Figure 4. Indicators of low treatment adherence (in absolute numbers) determined using the Moriski Green questionnaire after the introduction of the electronic program in patients living in a district with cardiovascular and respiratory diseases |
4. Conclusions
- The results obtained confirmed that the willingness of patients to seek treatment in all studied diseases in the district has changed qualitatively in a positive direction. These changes were mainly manifested in a significant increase in the high level of willingness to seek treatment and a decrease in the indicators of the group of patients with a low level. The fact that the medium level of willingness did not change significantly in a number of cases is due to the fact that some of the patients in this group were included in the high group, and on the contrary, some of the low group were included in the high group, and a smaller part in the medium group. The fact that the low level of willingness to seek treatment remained in an average of 25% of the observed patients can be attributed to various other reasons, in particular, the social status, education and work activities of the family. In accordance with the purpose of using the electronic program doriqami.uz to increase the willingness of patients to seek treatment in widespread chronic diseases. Its widespread application in practice will lead to a significant increase in the willingness of patients to seek treatment.