-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 755-760
doi:10.5923/j.ajmms.20261602.76
Received: Jan. 13, 2026; Accepted: Feb. 8, 2026; Published: Feb. 26, 2026

Improving Gradual Muscle Rehabilitation in the Period After Orthognathic Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShukhrat Boymuradov, Dilkhumor Quranbayeva
Department of Maxillofacial Surgery and Dentistry, Tahkent Medical State University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the development and implementation of comprehensive rehabilitation measures after orthognathic surgery in patients with dentoalveolar deformities. Based on international and domestic data from 2024–2025, key stages of preoperative, early, and late rehabilitation were defined. Special attention is given to ERAS protocols, myofunctional and speech therapy, nutritional support, and digital stability control. A model for implementing the rehabilitation pathway at the multidisciplinary clinic of Tashkent Medical State University is proposed. This study focuses on improving diagnostic approaches and orthodontic treatment outcomes for distal occlusion Class II Subclass II in children during the mixed dentition period. The research involved 42 patients aged 6 to 12 years who were divided into groups based on clinical forms of distal occlusion. Diagnostic methods included anthropometric measurements, radiographic analysis, and functional tests. Treatment protocols incorporated Twin block appliances, removable plates, elastopositioners, and fixed orthodontic systems. The findings demonstrate that functional appliances effectively stimulate mandibular advancement, normalize occlusal relationships, and enhance facial aesthetics. Early orthodontic intervention during the transitional dentition stage contributes to stable anatomical and functional outcomes and reduces the risk of relapse.
Keywords: Orthognathic surgery, Rehabilitation, Dentofacial deformities, ERAS, Myofunctional therapy, TMJ
Cite this paper: Shukhrat Boymuradov, Dilkhumor Quranbayeva, Improving Gradual Muscle Rehabilitation in the Period After Orthognathic Surgery, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 755-760. doi: 10.5923/j.ajmms.20261602.76.
1. Introduction
- The diverse range of clinical signs resulting from blockage in the rear part of the developed dental system, compounded by the frequent absence of first molars or damage to their chewing surfaces, poses challenges in both identifying and addressing the issue. Distal bite, a prevalent form of dental irregularity, involves not only morphological alterations but also various functional changes [1-3].Several orthodontic devices have been suggested for addressing distal deep bite with maxillary incisor retrusion. However, insufficient attention has been given to their design specifics, particularly those that facilitate altering the primary direction of jaw growth, including inducing posterior rotation in cases of horizontal growth. The treatment of distal occlusion alongside maxillary incisor retrusion lacks comprehensive examination, neglecting contemporary insights into dental system morphology, biomechanics, lower jaw kinematics, and soft tissue profile changes resulting from orthodontic interventions [6,9].Numerous uncertainties persist regarding the diagnosis and treatment of distal occlusion within the dental structure. Clear guidelines regarding the appropriate use of devices and the optimal timing of treatment based on the patient's age and the specific form of the anomaly are lacking. Furthermore, there is a notable absence of standardized protocols for diagnosing and treating distal occlusion in patients undergoing orthodontic treatment with fixed or removable appliances. The topic of retention also remains inadequately explored, with limited information available on the duration of the retention period and the types of retention devices utilized [5,7].Study Objective: Enhancing diagnostic techniques and orthodontic interventions for children undergoing tooth transition with distal occlusion (Class II, Subclass II), with the aim of attaining optimal anatomical and aesthetic outcomes.Distal occlusion refers to malocclusions in the sagittal plane, characterized by the lower dentition being positioned distally in relation to the upper dentition or vice versa, where the upper dentition is positioned mesially in relation to the lower. This condition disrupts the relationship of the teeth both in the anterior and lateral aspects [1,9,13].The primary diagnostic indicator for distal occlusion is the alignment of the posterior teeth according to Angle's Class II, where the mesiobuccal cusps of the upper first permanent molars are situated anteriorly to the intercuspal fissures of the corresponding lower first molars [2,8,17].Currently, distal occlusion stands out as one of the prevalent irregularities within the dental system, affecting a significant proportion of both young children and adolescents, with prevalence rates ranging from 37.3% to 65% among patients. Skeletal imbalances are recognized as one of the primary factors contributing to the development of a prognathic bite, which in turn disrupts the aesthetic harmony of the middle and lower facial zones.Many different factors play a role in the etiology of distal malocclusion. Among them are genetic predisposition, early tooth loss, anomalies and disorders of intrauterine development, injuries and diseases affecting growth and development, bad habits, as well as diseases of the upper respiratory tract that can interfere with normal nasal breathing [3,11,18].Orthodontic treatment is typically conducted during puberty, a period when bone growth tends to outpace the functional adaptation of muscles and ligaments. Consequently, there exists a heightened risk of juvenile arthropathy. It is therefore pertinent to evaluate not only the bone structures of the temporomandibular joint (TMJ) but also all its soft tissue components, including cartilage, articular disc, bilaminar zone, capsule, and masticatory muscles.According to modern views, one of the key aspects that determines the treatment strategy for patients with prognathic occlusion is the achievement of harmony between morphology and function. This implies ensuring the normal functioning of the dental-jaw system while maintaining physiological occlusion of the dentition and achieving a high level of facial aesthetics.In contemporary orthodontics, a significant issue revolves around identifying the optimal timing for initiating treatment. Numerous authors advocate commencing treatment after the eruption of premolars and second molars, as by this stage, the primary growth phase is largely complete. This approach facilitates more accurate outcome predictions and reduces the risk of relapse during the period of rapid facial skeletal growth. Conversely, some practitioners prefer to intervene during the transition of teeth, believing that early orthodontic intervention can influence the growth of cervical teeth and yield a more stable result with less exertion from both the practitioner and the patient, particularly in cases of skeletal distal occlusion [4,15,19].Removable orthodontic appliances have become very popular in the treatment of distal occlusion. Mechanically-acting removable orthodontic appliances and combined-action appliances are mainly used. Many authors give preference to functionally active and combined removable appliances that affect not only the dentition, but also soft tissues, indirectly affecting the bone structures and growth of the lower jaw.Currently, the most commonly utilized removable orthodontic appliances include inclined plane plates, the Andresen-Goipl activator, the Frenkel function regulator, the Bimler apparatus, and the Khurgina-Gulyaeva-Basharova apparatus. Inclined plane plates may not always yield the desired outcome, as children may inadvertently move their lower jaw behind the inclined plane when their jaw muscles fatigue. The Bimler bite former, while exerting pressure on the dentition during lower jaw movements, is susceptible to deformation and wire breakage at kinks due to its frame structure lacking fixation elements.The Frenkel function regulator, equipped with buccal shields and labial pads, alleviates lip and cheek pressure on underdeveloped alveolar processes and dentition areas [12,13,20].On the other hand, the Andresen-Goipl activator secures the lower jaw in the correct position and promotes its growth through multiple inclined planes, fostering normalization of masticatory and facial muscle function.Recently, orthodontic double-jaw structures composed of elastomeric materials have gained popularity. These structures effectively guide teeth into predetermined positions. For instance, a widely used removable orthodontic device known as a positioner offers universal effects on dentition. However, its creation involves labor-intensive methodologies, requiring specialized equipment in dental laboratories and skilled dental technicians. Consequently, standard positioners made of silicone materials have emerged in the orthodontic market. Their application facilitates the normalization of facial features and the establishment of correct occlusal contacts.The author of this study delineates that employing standard trainers leads to the normalization of incisor inclinations and alterations in sagittal and vertical dimensions of dentition, as well as dentoalveolar heights. Treatment with trainers aids in improving or even eliminating several dental anomalies while minimizing physical and psychological discomfort for the patient. Additionally, trainers can serve as retention devices, thereby reducing the likelihood of relapses. The author posits that standard trainers can streamline the process for clinicians by reducing the time required for patient examination and treatment [16-18].The primary category of functional devices employed to maintain the lower jaw in an anterior position consists of bimaxillary removable devices such as activators and function regulators. These devices artificially stimulate the muscles of the masticatory apparatus, altering the lower jaw's position and moving it anteriorly during distal occlusion. Utilizing removable structures enables the maintenance of a high level of oral hygiene for the child while also influencing the muscles of the maxillofacial region, thereby achieving a more stable treatment outcome.However, a significant drawback of double-jaw functional devices is their limited use to nighttime only, which reduces efficiency and prolongs the duration of active treatment for distal occlusion. A proposed alternative, the W.J. Clark twin-block device, overcomes this limitation. This device can be worn by the patient around the clock, even during meals. The ability to eat with the appliance in place allows for the utilization of masticatory forces to achieve a comprehensive functional response to treatment. The device is designed to position the lower jaw in protrusion and effectively modifies its growth through the action of leading planes incorporated into acrylic bite blocks.
2. Materials and Methods
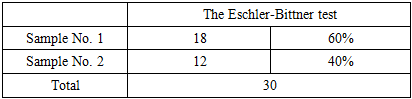
- We conducted a comparative analysis of orthodontic treatment involving 42 patients aged 6 to 12 years with distal occlusion of the dentition and class 2 anomalies in mixed dentition. These patients sought treatment at the multidisciplinary clinic of the Tashkent Medical Academy between 2023 and 2024. The patients were categorized into 4 groups:• Group: Patients with distal occlusion but without malocclusion in other planes (15 patients).• Group: Patients with distal occlusion combined with deep bite (12 patients).• Group: Patients with distal occlusion combined with open bite (3 patients).• Control group: Consisting of 12 patients.Anthropometric examinations (according to Korhaus and Pon), X-ray examinations (teleroentgenography and orthopantomography), functional examination methods (Eshler-Bitner test) and statistical examination methods were used in the patients.The first group (I) included 15 patients with distal pricus without abnormalities in other planes. Their treatment was carried out with the help of a brace system calculated from traditional methods and with the help of functional apparatus Twin-block.The second group (II) included 12 patients with distal pricus combined with deep pricus. They were treated with a removable plate for the upper jaw with an inclined chewing surface and a brace system.The third group (III) included 3 patients with distal pricus combined with open pricus. In them, the treatment was carried out with the help of functional kappa-elastopositioners, i.e. the myobrace system and the brace system.The fourth group (IV) is the control group. 12 children between 6-12 years of age, aesthetically satisfactory, maxillofacial and dental-jaw systems, as well as soft tissue parameters and cephalometric parameters, were taken.According to statistics, gender ratios were studied in the obtained groups and the following results were obtained:
|

3. Results
- The X-ray method of the study included the study, generalization and analysis of 42 radiographs, of which 8 were orthopantomograms and 34 were teleroentgenograms.The study of orthopantomograms of the jaws included determining the number of teeth; the presence, location and shape of permanent tooth buds; the degree of formation of their roots; determination of identification of dental defects; determination of the shape of the vomer, inferior nasal concha; dentoalveolar height in various parts of the dentition; depth of incisal overlap; as well as studying the condition of the TMJ, which is important for treatment planning.In 4 patients studied, underdevelopment of the lower jaw was found due to early removal of primary teeth in the lower jaw.1 patient had 3.4 adentia; 4.4 teeth on the lower jaw. We studied 22 teleroentgenograms of the head in a lateral projection with a prognathic bite before treatment of the patient. For a comparative study, 12 lateral teleroentgenograms of the head of patients with orthognathic occlusion from the control group were used.The study compared the dimensions studied in distal and orthognathic bites with the data of the norm.When deciphering telerengenograms, excessive development of the body of the upper jaw in length was found in 12 patients and varied within 3-5 mm. The size of the body of the upper jaw within normal limits was observed in 10 individuals. Underdevelopment of the body of the lower jaw in length was found in 18 patients, which varied with a difference from 5 to 7 mm. The size of the body of the lower jaw was found within normal limits in 12 individuals. However, in 4 patients there was an increase of 3-5 mm in the length of the body of the lower jaw. This indicated that the size of the jaws is a genetically determined structure.The position of the lower jaw relative to the upper jaw was determined by measuring the angles MM and A-B-SPP. Normally, these angles should be 90°. The MM angle indicated the position of the basal arches, that is, the body of the lower jaw, and the A-B-SPP angle indicated the position of its dentoalveolar part. This made it possible to differentiate the skeletal form from the dentoalveolar one. In 18 patients, a retroposition of the lower jaw was observed, in particular, a retroposition of its body 4°-19° more than normal was found in 12 individuals, and of the dentoalveolar part - in almost all patients. Thus, in 15 patients the retroposition of the body and dentoalveolar part prevailed, and in 3 patients only the dentoalveolar part. In addition to the position of the upper and lower jaws in the skull, we paid great attention to the axial inclination of the teeth. Thus, protrusion of the upper incisors was found in 16 individuals and ranged from 5° to 17° less than normal (65°), which corresponded to class II, subclass 1 according to Engle. At the same time, retrusion of the upper incisors was also observed in 4 patients, which varied from 6° to 12°, which corresponded to class II, subclass 2 according to Engle. A diagnostic functional test was carried out in all patients we studied. To do this, the patient must close the teeth in the usual occlusion and remember the profile shape. Patients were then asked to move the mandible forward until the posterior teeth were neutral.In 60% of those studied, the facial profile improved when the lower jaw was shifted forward, which was due to underdevelopment of the lower jaw. (Sample No. 1).In 40% of those studied, the facial profile worsened when the lower jaw shifted forward, the reason for this being the excessive development of the upper jaw and its predominance over the lower jaw. (sample No. 2).
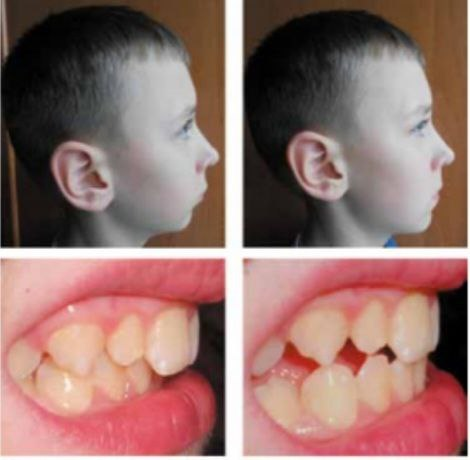 | Figure 1. Carrying out the Eschler-Bittner test on a 12-year-old patient with a distal bite (test No. 1) |
|
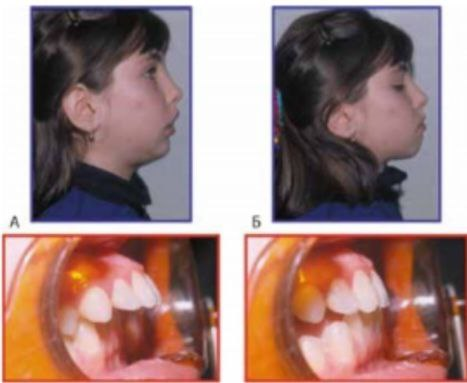 | Figure 2. Carrying out the Eschler-Bittner test in an 11-year-old patient with a distal bite (test No. 2) |
4. Discussion
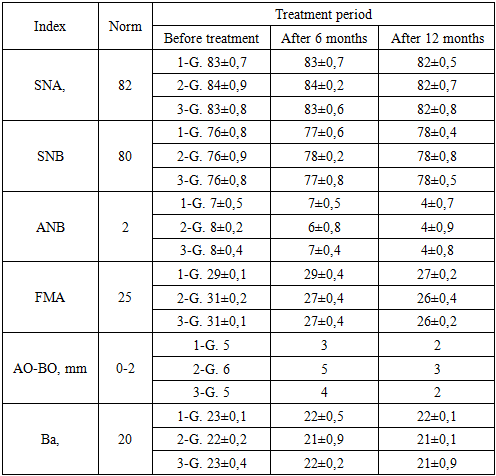
- Patients in group 1 were prescribed the Twin-block method, a contemporary approach for correcting this anomaly. The Twin-block, initially proposed by Clark and later modified, comprises two main components. Its primary active element is an expanding screw fitted onto the upper jaw. This device operates by encouraging the lower jaw to assume a corrective position. Being detachable, patients swiftly adapted to wearing them consistently, even during meals. This rapid adaptation resulted in fewer treatment interruptions and quicker achievement of positive outcomes. The constructive bite mechanism, which holds the lower jaw in a protruded position, also enhances facial aesthetics.Treatment proceeded in two stages: First, active treatment involved advancing the lower jaw while normalizing the occlusal relationship vertically. Second, maintaining correct incisor closure during the pre-eruption period of lateral teeth involved using a plate on the upper jaw with an anterior inclined biting platform and multiple clasps. The inclined bite platform extended to the distal areas, ending at the level of the distal surface of the lower jaw canines. To eliminate deep incisal overlap, occlusal pads were ground using an upper jaw apparatus for dentoalveolar lengthening at lower jaw molar areas. This grinding occurred a week after device fitting and patient adaptation. It gradually created free space on the lower jaw molars' chewing surfaces, approximately 1-2 mm, to prevent tongue displacement in the newly formed gaps.In cases of insufficient lower jaw growth rate or vertical jaw growth type, we monitored lower jaw advancement by adding self-hardening plastic layers on the inclined slopes of the upper jaw plate. As evident from the tables, distal occlusion occurrence in the observed children correlates with the distal position and/or delayed growth and development of the lower jaw. Bittner-Eschler tests yielded positive results in all 15 patients in the first group (100%), confirming the obtained cephalometric indicators and indicating the appropriateness of treatment with functional methods.In the 2-group of patients under study, plates were installed on their jaws. Because they had a distal anomaly combined with a deep pricus, the pricus height was raised with the help of plates and braces were worn.Children primarily wore the device during nighttime and for 2-3 hours in the afternoon, thereby naturally prolonging the treatment duration. Additionally, the bulkiness of the design, with its numerous components, often posed a challenge for patients. It's worth noting that in patients using the Frenkel function regulator, monitoring the posterior height of the lower face becomes challenging. As orthodontic treatment occurs during the child's active growth phase, the function regulator needs to be replaced several times throughout the treatment course, typically requiring the production of 2-3 devices.In the third group, the treatment of patients with distal anomalies combined with an open pricus was studied. Myobrace system - elastopositioners were used in them.The MYOBRACE (MBS) system is designed to condition the muscles of the maxillofacial area, aiding in the correction of teeth alignment. Unlike other elastopositioners, they feature high walls and indentations for both upper and lower dental arches, guiding emerging teeth during their eruption. The MYOBRACE (MBS) orthodontic appliance series is employed for treatment due to its versatility, eliminating the need for additional orthodontic appliances. Moreover, this system can serve as a pre-finisher with a retainer following braces removal, as well as for correcting various types of occlusal discrepancies.The obtained results can be compared in the following table (Table 3):
|
 | Figure 3 |
5. Conclusions
- Each functional device comes with its own set of advantages and drawbacks. It's crucial to accurately diagnose, predict, control, and manage the type of growth, which enhances the effectiveness of orthodontic treatment for children with distal occlusion during early mixed dentition using functional methods.In conclusion, conducting the Bitner-Eschler clinical test alongside clinical and cephalometric indicators offers insights into the primary role of the upper or lower jaw in the development of this malocclusion. The ability to manage vertical growth enables orthodontists to choose between functional devices, favoring either a Frenkel regulator or a Twin-block.A well-thought-out approach to planning the treatment of distal occlusion in children has led to improvements in smile aesthetics, the ability to monitor and manage jaw bone growth, elimination of bad habits, normalization of breathing, significant reduction, and in some cases, elimination of the need for future dental surgery in treating this malocclusion.