-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 731-736
doi:10.5923/j.ajmms.20261602.71
Received: Jan. 6, 2026; Accepted: Feb. 2, 2026; Published: Feb. 26, 2026

Clinical and Pathomorphological Profile of Polypoid Rhinosinusitis Developing After Nasal Septal Trauma
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYuldashev Kahramonjon Shukurjon ugli1, Mahkamov Nosirjon Juraevich2
1Fergana Public Health Medical Institute, Independent Researcher, Uzbekistan
2Andijan State Medical Institute, DSc, Professor, Uzbekistan
Correspondence to: Yuldashev Kahramonjon Shukurjon ugli, Fergana Public Health Medical Institute, Independent Researcher, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Post-traumatic polypoid rhinosinusitis, which develops following nasal septal trauma, is a common inflammatory disorder affecting the nasal cavity and paranasal sinuses. Its histopathological characteristics are critical for identifying the morphological features of polyp formation and inflammatory processes in nasal tissues. This study analyzes the histological changes observed in post-traumatic polypoid rhinosinusitis, including epithelial hyperplasia, stromal lymphocytic and plasmacytic infiltration, fibrosis, and vascular remodeling. Immunohistochemical analysis further elucidated the distribution and activity of immune cells involved in the inflammatory response. Age and sex were found to influence the severity and pattern of morphological alterations: younger patients demonstrated pronounced inflammatory infiltration and epithelial proliferation, middle-aged patients exhibited increased fibrotic remodeling, and older patients primarily showed stromal fibrosis with reduced inflammation. Male patients were more frequently affected than females, with the highest prevalence observed in the 23–33-year age group. Histological assessment provides essential insight into the clinical presentation, progression, and potential complications of post-traumatic polypoid rhinosinusitis. This study contributes valuable information to support early diagnosis, targeted therapeutic strategies, and clinical decision-making for otorhinolaryngologists and clinical researchers.
Keywords: Polypoid rhinosinusitis, Nasal septal trauma, Histopathology, Inflammation, Fibrosis, Age-related changes, Immunohistochemistry
Cite this paper: Yuldashev Kahramonjon Shukurjon ugli, Mahkamov Nosirjon Juraevich, Clinical and Pathomorphological Profile of Polypoid Rhinosinusitis Developing After Nasal Septal Trauma, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 731-736. doi: 10.5923/j.ajmms.20261602.71.
1. Introduction
- Chronic rhinosinusitis with nasal polyps (CRSwNP) is a persistent inflammatory condition characterized by swelling of the sinonasal mucosa and formation of polyps, leading to significant impairment in quality of life, including nasal obstruction, rhinorrhea, and olfactory dysfunction [1,2]. The pathogenesis of CRSwNP involves persistent mucosal inflammation and tissue remodeling, which necessitates detailed clinical and histopathological evaluation for understanding disease progression and optimizing treatment [3,4]. Histopathological studies have demonstrated that nasal polyp tissues frequently exhibit eosinophilic infiltration, epithelial hyperplasia, and stromal remodeling, which are key indicators of chronic inflammatory processes and correlate with disease severity [5,6].Structured classification of nasal polyps into eosinophilic, fibrous, and mixed inflammatory subtypes has provided insights into the heterogeneous nature of CRSwNP and informs personalized management strategies [1,4]. Quantitative assessments of eosinophil counts and goblet cell hyperplasia have been shown to correlate with clinical severity, risk of recurrence, and the need for revision surgery [5,7]. Additionally, studies highlight that tissue eosinophilia and stromal remodeling are fundamental features underlying disease pathogenesis and recurrence, emphasizing the importance of precise histopathological analysis in guiding therapeutic decisions [3,6].Furthermore, sinonasal polyps often coexist with comorbid conditions such as asthma and allergic rhinitis, which contribute to systemic and local inflammatory responses, impacting disease severity and treatment outcomes [8,9,10]. Longitudinal analyses of histopathological changes demonstrate variable inflammatory cell patterns over time, reinforcing the need for continual morphological evaluation in both primary and recurrent CRSwNP cases [11,12]. Collectively, these findings underscore the clinical relevance and scientific significance of studying the morphological characteristics of polypoid inflammation, including post-traumatic polypoid rhinosinusitis, to improve diagnostic accuracy and optimize patient-specific therapeutic strategies [1,12].Purpose of the StudyTo investigate the clinical and pathomorphological features of posttraumatic nasal polyposis and, thereby, to elucidate the morpho-functional mechanisms of the disease and provide a scientific basis for improving diagnostic and therapeutic strategies.
2. Material and Methods
- The study included 121 patients (76 males and 45 females) aged 12 to 70 years who were treated for post-traumatic nasal polyposis at the Fergana Regional Pathology Bureau between 2020 and 2024. Patients were categorized into five age groups: 12–22, 23–33, 34–44, 45–55, and 56–70 years. The largest proportion of patients belonged to the 23–33 years age group (41.3%), while the smallest proportion was in the 56–70 years group (4.1%).Clinical data, including age, sex, disease duration, and main morphological types of nasal polyps, were collected from hospital records. Hospitalization duration ranged from 0–1 day to 8–15 days, with the majority of patients treated for 4–7 days (34.7%).For histopathological analysis, tissue samples measuring 1.5 × 1.5 cm were obtained from the nasal polyps. Specimens were fixed in 10% neutral buffered formalin for at least 48 hours. Following fixation, tissues were dehydrated, cleared, and embedded in paraffin. Sections of 4-5 μm thickness were prepared and stained with hematoxylin-eosin. Histopathological examination was performed using a ZEISS Primo Star microscope. Morphological analysis focused on epithelial hyperplasia, stromal lymphocytic and plasmacytic infiltration, fibrosis, and vascular remodeling.
3. Results
- During the study, the clinical and histopathological features of post-traumatic polypoid rhinosinusitis were investigated in 121 patients treated at the Fergana Regional Bureau of Pathological Anatomy between 2020 and 2024. Based on age, sex, and medical history, the patients were stratified into five age groups: Group 1, 12-22 years, Group 2, 23–33 years, Group 3, 34-44 years, Group 4, 45-55 years, and Group 5, 56-70 years. The results indicated that the highest prevalence of post-traumatic polypoid rhinosinusitis occurred in Group 2 (23-33 years), accounting for 41.3% of the total cases. The lowest prevalence was observed in Group 5 (56–70 years), with only 5 patients (1 female and 4 males) affected. The remaining age groups exhibited intermediate prevalence rates (see Figure 1).
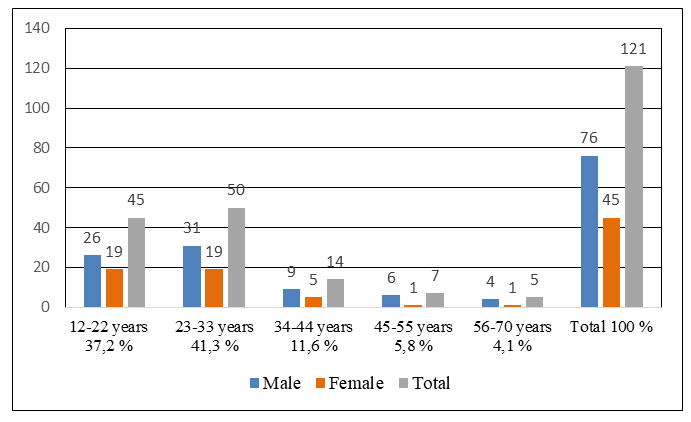 | Figure 1. Distribution of patients with post-traumatic nasal polyposis included in the planned study. Analysis based on age, sex, and incidence (%) |
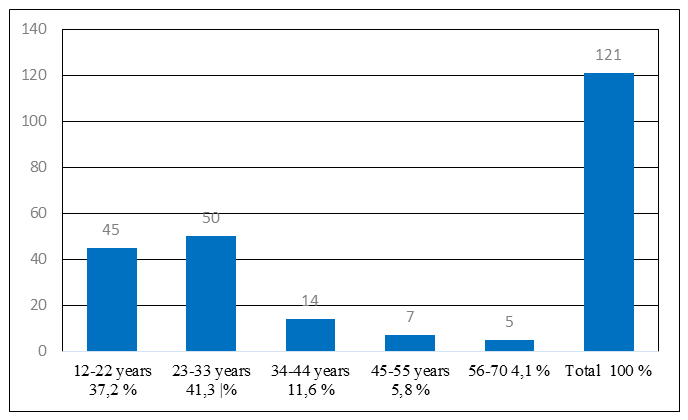 | Figure 2. Age distribution of patients with posttraumatic polypoid rhinosinusitis, expressed as percentage of total cases |
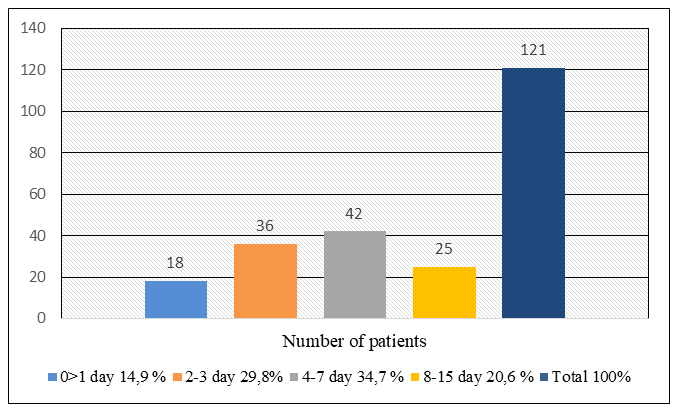 | Figure 3. Distribution of patients by duration of hospital stay (%) |
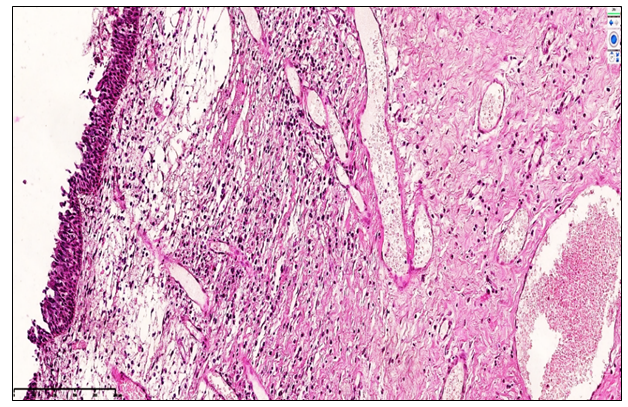
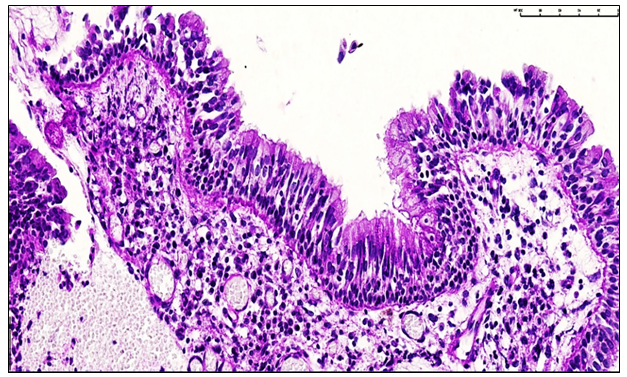 | Figure 4. Chronic polypoid rhinosinusitis, 1.5 years post-nasal trauma. Focal epithelial hyperplasia and lymphoid cell infiltration are observed in the mucosal lining, with sparse neutrophils. Interstitial edema is present among lymphocytes in the glandular stroma. Staining: H&E, magnification ×100 |
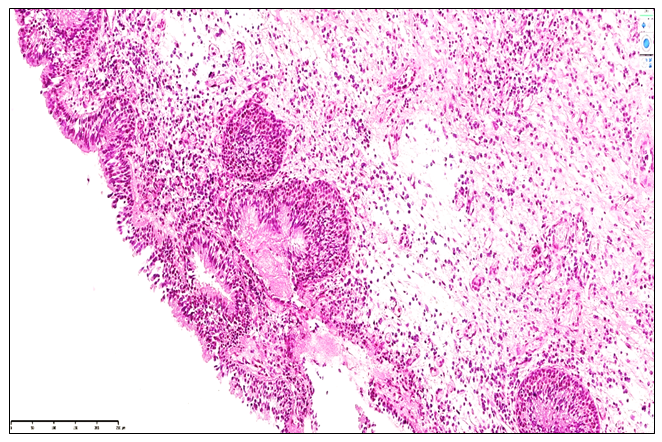
 | Figure 5. Chronic fibrotic nasal polyposis, Group 2 (1.7 years post-nasal trauma): The covering epithelium of the nasal mucosa exhibits mild hyperplasia and focal lymphocytic infiltration, with a sparse presence of neutrophils. Within the glandular stroma, cystic dilations and signs of vascular congestion are observed. Staining method: H&E, magnification 10×10 |
 | Figure 6. Chronic polypous rhinosinusitis, Group 3. At 3.5 years post-nasal trauma, the nasal mucosa epithelium exhibits atrophy, desquamation, and focal lymphocytic infiltration. In the glandular stroma, interstitial swellings are observed among lymphocytes. Staining: H&E; Magnification: 10×10 |
4. Conclusions
- The present study comprehensively analyzed the clinical and pathomorphological features of post-traumatic polypoid rhinosinusitis, providing critical insight into the morphofunctional alterations occurring in the nasal mucosa following nasal septal injury. The findings demonstrate that post-traumatic nasal polyposis predominantly affects young and middle-aged male patients, with the highest prevalence observed in the 23–33-year age group. This demographic trend likely reflects increased exposure to physical activity, domestic injuries, and trauma-related risk factors in this population.Histopathological evaluation revealed a temporal progression of mucosal changes, corresponding to the duration post-trauma. Early stages (1–1.5 years) were characterized by active serous inflammation, epithelial hyperplasia, and sparse stromal fibrosis, reflecting initial reparative and adaptive processes. Intermediate stages (1.5–3 years) demonstrated moderate epithelial metaplasia, proliferation of immune cells, lymphoid MALT hyperplasia, and vascular congestion, indicative of adaptive remodeling and a gradual decline in inflammatory reactivity. In the late stages (3–5 years), chronic polypoid rhinosinusitis exhibited pronounced atrophic, fibrotic, and sclerotic alterations. These included epithelial flattening, extensive stromal fibrosis, cystic glandular changes, neoangiogenesis, and hyporeactive lymphoplasmacytic infiltration, collectively demonstrating a progressive decline in mucosal morphofunctional integrity and mucociliary clearance.The study underscores that post-traumatic polypoid rhinosinusitis is a dynamic disease process, wherein age and duration post-injury are key determinants of the severity and nature of morphological alterations. Younger patients exhibited more pronounced inflammatory responses and epithelial proliferation, while middle-aged and older patients were more prone to fibrotic remodeling and glandular atrophy. These findings highlight the importance of longitudinal monitoring of patients with nasal trauma, as structural remodeling and hyporeactive chronic inflammation may predispose to persistent nasal obstruction, impaired mucociliary transport, and secondary infectious complications.Additionally, the identification of hyporeactive chronic inflammation, cystic glandular dilation, and stromal fibrosis provides a histopathological basis for the reduced efficacy of conservative treatments in late-stage post-traumatic nasal polyposis. The study emphasizes the need for early diagnosis and timely intervention to prevent irreversible structural changes and optimize therapeutic outcomes. Immunohistochemical and morphometric evaluations further support the concept that targeted management strategies should consider both the inflammatory and structural components of the disease, particularly in patients with prolonged post-traumatic evolution.In conclusion, this investigation provides a comprehensive clinical and pathomorphological framework for understanding post-traumatic polypoid rhinosinusitis. The detailed correlation between patient demographics, post-trauma duration, and mucosal remodeling advances the scientific understanding of disease progression and establishes an evidence-based foundation for the development of personalized diagnostic and therapeutic strategies in otorhinolaryngology. These findings not only enhance clinical decision-making but also inform future research on the prevention, management, and long-term outcomes of post-traumatic nasal polyposis.