-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 728-730
doi:10.5923/j.ajmms.20261602.70
Received: Jan. 4, 2026; Accepted: Feb. 3, 2026; Published: Feb. 26, 2026

Clinical and Immunological Characteristics of Cognitive Disorders in Children with Delayed Speech Development
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBerdieva Khilolakhon Umarjonovna
PhD Student, Department of Neurology, Pediatric Neurology and Medical Genetics of the Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Berdieva Khilolakhon Umarjonovna, PhD Student, Department of Neurology, Pediatric Neurology and Medical Genetics of the Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Ninety children aged 3–7 years were examined and stratified into two groups. The first group consisted of children with delayed speech development (DSD) in combination with attention-deficit/hyperactivity disorder (ADHD), while the second group included children with DSD due to residual-organic brain lesions (ROL). Children with DSD associated with ADHD demonstrated a significantly higher speech development coefficient (24.9 ± 3.9) compared with those with residual-organic brain pathology (17.7 ± 6.7; p < 0.001). This finding suggests a more favorable functional prognosis in cases of predominantly functional speech impairment. Conversely, children with residual-organic brain lesions exhibited more severe neurological and cognitive deficits, reflecting delayed cerebral maturation and decreased functional activity of cortical structures.
Keywords: Delayed speech development, ADHD, Residual-organic lesions, Children, Speech function, Cognitive development
Cite this paper: Berdieva Khilolakhon Umarjonovna, Clinical and Immunological Characteristics of Cognitive Disorders in Children with Delayed Speech Development, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 728-730. doi: 10.5923/j.ajmms.20261602.70.
Article Outline
1. Introduction
- In contemporary pediatric neurology, delayed speech development (DSD) is regarded as one of the most prevalent neuropsychological disorders of early childhood. Speech acquisition represents a complex, multilevel, and multifactorial process that relies on physiological mechanisms and is closely influenced by social, cultural, and psychological factors [7,9].Speech development is particularly vulnerable to adverse influences, and its impairment often leads to substantial consequences, including difficulties in cognitive functioning and communicative activity, as well as deviations in neuropsychological and social development. These effects are especially pronounced in early childhood, a critical period during which the foundational mechanisms of speech are formed and determine its subsequent maturation [2,4].In recent years, speech disorders in children have become a major concern for professionals across multiple disciplines, including pediatric neurologists, speech therapists, psychologists, and educators. This heightened attention is обусловлено not only by the increasing prevalence of DSD but also by the challenges associated with its early identification and timely intervention. According to various studies, the prevalence of delayed speech development in children ranges from 5% to 25% [1,6].From an etiological perspective, DSD may arise from both organic and functional causes. Organic factors primarily include perinatal central nervous system injury, traumatic brain damage, neuroinfections, cerebral palsy, epilepsy, neurosensory hearing loss, and other pathological conditions. These disorders affect brain structures involved in the regulation of motor and cognitive functions, thereby impeding normal speech development [3,7,8].Conversely, functional forms of delayed speech development are more frequently associated with unfavorable psychoemotional environments, impaired parent–child communication, limited linguistic stimulation, and pedagogical neglect [2,5].Purpose of the ResearchThe objective of this study was to characterize the clinical and neurological features of delayed speech development (DSD) in children, to examine the association between the etiology of speech delay and neurological status, and to identify prognostic indicators distinguishing functional from organic speech disorders. Additionally, the study sought to define clinical criteria that may support early diagnosis and timely therapeutic intervention, thereby enhancing the effectiveness of neurodevelopmental rehabilitation in affected children.Objective is to identify the clinical and neurological characteristics of delayed speech development in children and to assess the relationship between the type of speech disorder and neurological status across different etiological forms.
2. Materials and Methods
- The study was carried out at the clinic of the Tashkent Pediatric Medical Institute. Ninety children aged 3–7 years diagnosed with delayed speech development were examined. The participants were equally allocated into two groups.Group I (n = 45; 50%) comprised children with delayed speech development (general speech underdevelopment, level II) associated with attention-deficit/hyperactivity disorder (ADHD).Group II (n = 45; 50%) included children with delayed speech development (general speech underdevelopment, level II) resulting from residual-organic brain lesions (ROL).In addition, a control group consisting of 15 age- and sex-matched children without speech impairments was included in the study.
3. Results
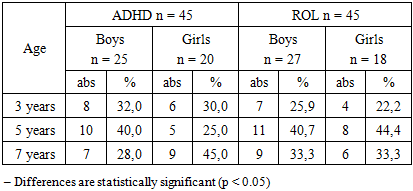
- To characterize the age and sex distribution of the examined children, both clinical groups were analyzed according to these variables (Table 1). The resulting data made it possible to identify the age periods in which delayed speech development was most prevalent and to assess potential differences between children with ADHD-associated and residual-organic forms of speech delay.
|
|

4. Discussion
- Children whose delayed speech development is associated with attention deficit hyperactivity disorder demonstrate a significantly higher speech development coefficient (24.9 ± 3.9) than children with residual-organic brain damage (17.7 ± 6.7), which indicates a more favorable functional prognosis in non-organic forms of DSD. In contrast, children with organic cerebral lesions show more severe neurological and cognitive deficits, reflecting delayed cortical maturation and decreased functional activity of brain structures. Timely identification of speech delay and early corrective interventions play a key role in improving rehabilitation outcomes and in preventing the development of persistent speech and cognitive impairments.
5. Conclusions
- Children with delayed speech development in the context of attention deficit hyperactivity disorder have a significantly higher speech development coefficient (24.9 ± 3.9) compared with children suffering from residual-organic brain lesions (17.7 ± 6.7), which points to a more favorable functional prognosis in non-organic variants of DSD. Conversely, organic brain pathology is associated with more pronounced neurological and cognitive disturbances, indicating delayed cortical maturation and reduced functional activity of cerebral structures. Early detection of speech delay and timely implementation of corrective interventions are crucial for enhancing rehabilitation effectiveness and for preventing the persistence of speech and cognitive deficits.
ACKNOWLEDGEMENTS
- The author sincerely thanks the staff of the Department of Neurology, Pediatric Neurology, and Medical Genetics of Tashkent State Medical University for their professional support, valuable recommendations, and guidance throughout the research. Special appreciation is extended to the children who participated in the study and to their parents for their trust and cooperation. The author is also grateful to colleagues from the university clinic for their assistance in conducting clinical assessments and laboratory investigations, which contributed significantly to the completion of this work.