Rasulova Raykhon
Termez Branch of Tashkent State Medical University, Termez, Uzbekistan
Correspondence to: Rasulova Raykhon, Termez Branch of Tashkent State Medical University, Termez, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Currently, the study of the mechanisms of comorbidity formation in patients is one of the relevant areas of scientific research. In pathological conditions leading to a weakened immune system, the herpes virus can manifest in comorbid forms. Its pathogenesis involves central and peripheral sensitization of the nervous system, which is accompanied by persistent neuroimmune inflammation of the ganglia and spinal cord fibers, as well as impaired conduction of nerve fibers. As a result of demyelination, herpes and other autoimmune diseases can combine, causing a comorbid condition. All this served as an incentive to develop measures aimed at simplifying the diagnosis of the features of the course of postherpetic trigeminal neuralgia. The information presented in the work allows doctors to use it in their practice to make a correct and accurate diagnosis for patients with PHTN, which, in turn, contributes to the effective organization of treatment and the achievement of medical results.
Keywords:
Herpes, Trigeminal nerve, VAS, Pain Detect, DN4, MFI-20, SF-36
Cite this paper: Rasulova Raykhon, Features of Trigeminal Neuralgia in Comorbid Herpetic Infection, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 665-669. doi: 10.5923/j.ajmms.20261602.57.
1. Introduction
To date, there is no consensus regarding the clinical and laboratory markers of postherpetic neuralgia. Herpes is not only a cosmetic problem due to various skin rashes but also a serious medical problem, as it can cause severe complications. Neuralgia in herpes infection is a common and difficult-to-treat complication [1,2,3,4,5,6,7]. Various mechanisms are involved in the pathogenesis of neuralgia in herpes infection. The transmission of pain signals is impaired in the affected nerve, leading to increased activity of overlying neurons (hyperalgesia). Ectopic activity develops in the affected area or along the nerve fiber. Pain in trigeminal neuralgia in comorbid herpes infection can be intense, stabbing, accompanied by burning, and can be unbearably painful, which significantly worsens the patient's quality of life and reduces their ability to work. The pain is usually unilateral and rarely spreads to the other side [8,9,10,11,12].
2. Purpose of the Research
To study the clinical features of trigeminal neuralgia in comorbid herpes infection and to improve diagnosis.
3. Materials and Methods
The main group included 82 patients with positive results for HSV IgG types 1 and 2, CMV IgG by ELISA, with comorbid herpes infection trigeminal neuralgia. The comparison group consisted of 39 patients with trigeminal neuralgia of other etiologies and 21 healthy individuals.Clinical indicators of patients, pain intensity, quality of life, results of laboratory tests. To assess the neuropathic nature of pain, the Pain Detect and DN4 scales were used. The Hamilton scale was used to assess anxiety. For the subjective assessment of asthenia, the MFI-20 scale was used, and for quality of life, the SF-36 questionnaire. The obtained results were subjected to statistical processing, including the calculation of average relative values and their errors. Student's t-test and the chi-square test were used to assess differences between groups and their significance.
4. Results and Discussion
The average age of the patients participating in the study in the main, comparison, and control groups was 39.5±1.6, 47.2±2.7, and 27.8±1.2 years, respectively (p<0.05) (Fig. 1).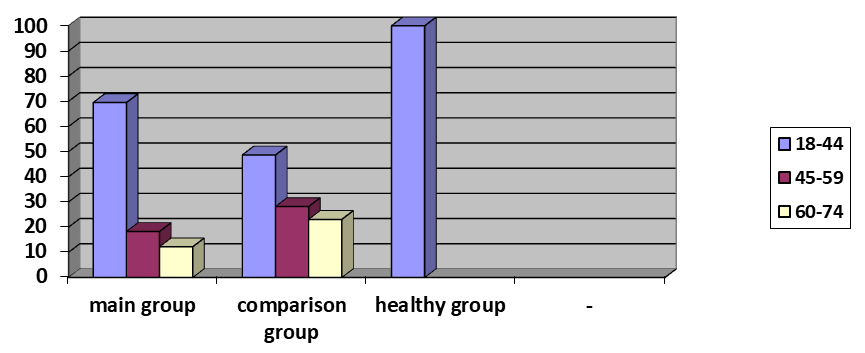 | Figure 1. Distribution of Patients by Age Groups (%) |
Women predominated among the patients in all three groups. The proportion of men was 26.8% in the main group, 20.5% in the comparison group, and 47.6% in the healthy group, with no statistically significant differences between the groups identified.The results showed that in the main group with trigeminal neuralgia in comorbid herpes infection, 59.8% of patients had pain predominantly on the right side of the face, while 40.2% of patients had pain on the left side. In the comparison group with trigeminal neuralgia, the situation was opposite: 41% of patients had pain on the right side, and 59% had pain on the left side of the face. Thus, it can be concluded that in patients with trigeminal neuralgia in comorbid herpes infection, pain is most often localized on the right side of the face.The localization of pain in specific areas of the face plays an important role in the correct diagnosis of the disease and the choice of appropriate treatment tactics. Therefore, in our study, we analyzed in which specific areas of the face the pain is observed. It turned out that in patients with trigeminal neuralgia in comorbid herpes infection, the pain was predominantly localized in the forehead and upper part of the face (86.6%), with the eye area being the second most common (36.6%). Furthermore, 37.8% of patients had pain in two or more areas of the face simultaneously.In patients from the comparison group with trigeminal neuralgia, unlike the main group, pain was most often observed in the area of the lower jaw and ear (59.0%), as well as the upper jaw (41.0%). Thus, it can be concluded that in patients with trigeminal neuralgia in comorbid herpes infection, pain is predominantly localized in the forehead, upper face, and eye areas.Analysis of patient complaints revealed factors that increase pain, which were studied and assessed. In the main group, these factors were: washing the face (62.2%), touch of clothing or a pillow (47.6%), exposure to wind (78%), as well as the influence of two or more factors simultaneously (87.8%). In the comparison group, these figures were 56.4%, 59%, 61.5%, and 56.4%, respectively. However, a statistically significant difference (p<0.001) was found only among patients who were affected by two or more factors.In all patients from the main and control groups, the exit point of the trigeminal nerve (Valleix's points) was painful. Upon analysis of which specific branch of the fifth cranial nerve was damaged, it turned out that in the majority of patients in the main group, the first branch was damaged, while in patients in the control group, the third branch was damaged (p<0.001) (Fig. 2). 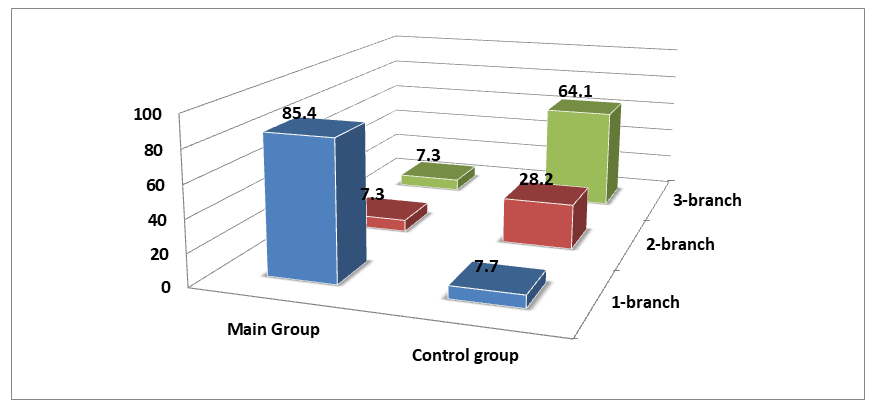 | Figure 2. Distribution of Patients by Damage to the V Pair of Nerve Branches (%) |
When analyzing the affected side of the face and the nerve branches in patients in the main group diagnosed with postherpetic trigeminal neuralgia, the data presented in Figure 3 were obtained.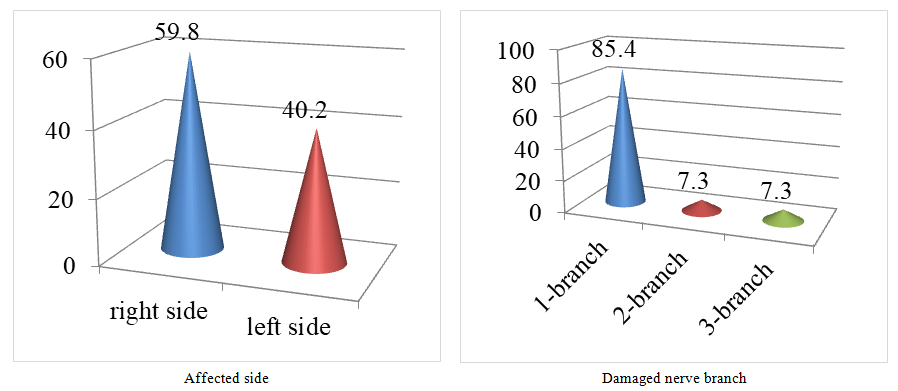 | Figure 3. Distribution of Patients in the Main Group by Facial Side with Damage and Damaged Nerve Branch (%) |
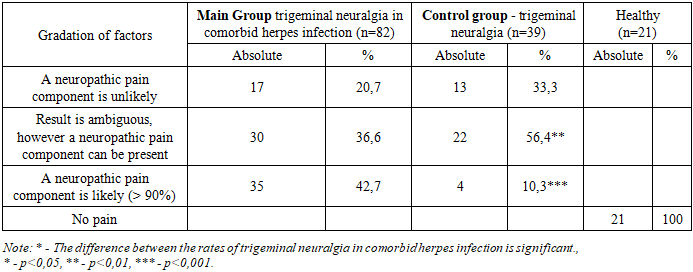
The obtained results show that lesions on the right side are more common than on the left. Among the branches of the fifth cranial nerve, damage to the first branch is most often observed.When studying pain using the PainDetect scale, almost half of the patients in the main group (42.7%) had a high probability of a neuropathic component of pain, while more than half of the patients in the control group had an uncertain result, but also a probability of having a neuropathic component of pain (Table 1).Table 1. Distribution of Patients by PainDetect Results (%)
 |
| |
|
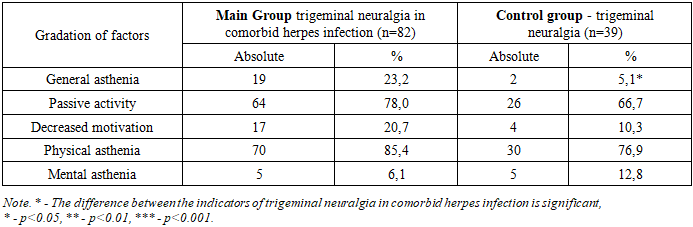
When analyzing the results of the DN4 scale, all patients in the main group answered "yes" to 4 or more questions. In the control group, 66.7% answered "yes" to 4 or more questions, and 33.3% answered "no" to fewer than 4 questions; in the group of healthy people, all patients answered "no" to all questions (p<0.001).The Hamilton scale was used to assess anxiety. According to the obtained results, patients in the main group had no anxiety (0-7 points). All patients in the healthy group had no anxiety, and in the control group, 35.9% had no anxiety. Mild anxiety (8-19 points) was detected in 52.4% of patients in the main group and 51.3% of patients in the control group. Patients with severe anxiety (20 points and above) accounted for 47.6% in the main group, which is 3.7 times higher compared to the control group (12.8%) (p<0.001).Table 2. Distribution of Patients by MFI-20 Scale
 |
| |
|
The obtained results show that the majority of patients in both groups experience reduced activity and physical asthenia. Mental asthenia is more common among patients in the control group than in the main group, but no statistically significant difference was found. The proportion of patients with general asthenia in the main group was 4.5 times higher than in the control group (p<0.001).When studying the quality of life using the SF-36 questionnaire, the average scores of the main and comparison groups statistically significantly differed from the group of healthy individuals in terms of mental and physical health components (p<0.001) (Fig. 4).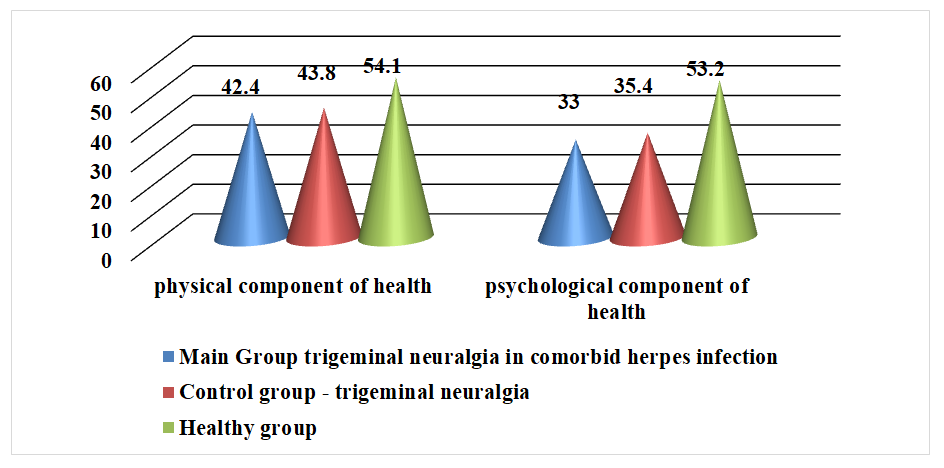 | Figure 4. Distribution of Patients by SF-36 Results |
In the main group, the average platelet count was 240.96•10^9/L, in the comparison group this indicator was somewhat higher (290±2.5•10^9/L). In 19 (23.2%) patients of the main group, platelet counts were below normal. In 70 (85.4%) patients of the main group, ESR results were above normal, compared to 10 (25.6%) patients in the comparison group (p<0.001). The mean ASLO values in the main, control, and healthy groups were 303.2±5.6, 214.1±3.72, and 171.0±4.3, respectively. The mean values of these indicators in the groups differed significantly (p<0.001). All healthy participants had ASLO below 200. In 25.6±7.0% of patients in the control group, the ASLO indicator was below 200, and in the rest, it was higher. All patients in the main group had ASLO above 200.The results of the study demonstrated that patients with postherpetic trigeminal neuralgia have significant deviations in clinical and laboratory parameters. A high frequency of pain in the forehead and upper face, as well as increased sensitivity to external stimuli, was revealed. Comparison of the data with existing studies confirms the relevance of using an integrated approach in diagnosis.
5. Conclusions
Based on the analysis of clinical and laboratory data of patients with herpetic trigeminal neuralgia and trigeminal neuralgia of other etiologies, the following conclusions can be drawn:1. In patients with trigeminal neuralgia in comorbid herpes infection, pain is observed in 60% of cases on the right side of the face, while in the control group, the opposite picture is observed. In patients with trigeminal neuralgia in comorbid herpes infection, pain is mainly localized in the forehead and eye areas.2. In patients with trigeminal neuralgia in comorbid herpes infection, the 1st branch of the fifth pair of cranial nerves is more often affected.3. Mental asthenia is more common among patients in the control group than in the main group; however, no statistically significant difference was found. The proportion of patients with general asthenia in the main group was 4.5 times higher than in the control group.4. When assessing the quality of life using the SF-36 questionnaire, the average scores of the main and comparison groups statistically significantly differed from the group of healthy individuals in terms of mental and physical health components.
References
| [1] | Avijgan M, Hajzargarbashi ST, Kamran A, Avijgan M. Postherpetic Neuralgia: Practical Experiences Return to Traditional Chinese Medicine. // J Acupunct Meridian Stud. 2017 Jun; 10 (3): 157-164. |
| [2] | Herpetic Lesions of the Peripheral Nervous System. Lecture (Third Report). Treatment of Herpetic Ganglionitis and Postherpetic Neuralgia. / Yu.N. Sorokin. // International Neurological Journal. - 2015. - No. 3 (73). - P. 68-75. |
| [3] | Eshmolov Sergey Nikolaevich, Klimovitskaya Elizaveta Genrikhovna, Kuzmina Maria Nikolaevna, Sitnikov Ivan Germanovich. Lesions of the Nervous System in Herpesvirus Infections // Children's Infections. 2022. No.4 (81). |
| [4] | Karakulova Yulia Vladimirovna, Kirichenko Svetlana Aleksandrovna. Quality of Life of Patients with Neuropathic Pain Syndrome after Herpes Zoster // Journal Medial. 2013. No.2 (7). |
| [5] | Kiparisova Ya.S. Trigeminal Neuralgia: Etiology, Pathogenetic Mechanisms (Literature Review) // Clinical Neurology. ˗ 2020. ˗ No. 1. ˗ P. 28-31. |
| [6] | Mavrov G.I., Zapolsky M.E. Epidemiology of Herpetic Infection and Herpes-Associated Diseases // Ukrainian Journal of Dermatology, Venereology, Cosmetology. ˗ 2013. ˗ No. 2 (49). ˗ P. 17-22. |
| [7] | Characteristics of Pain and Neurological Status of Patients with Comorbid Herpetic Trigeminal Neuralgia. / Rasulova R.P., Kuranbaeva S.R. // ISSN 2181-0982 Journal of Neurology and Neurosurgical Research. Tashkent: No. 5/2024. 12-16. |
| [8] | Features of the Neurological Status of Patients with Trigeminal Neuralgia with Comorbid Herpes Infection. / Rasulova R.P., Kuranbaeva S.R. // ISSN 2181-5534 Infection, Immunity and Pharmacology. Tashkent: No. 6/2023. 110-117. |
| [9] | Features of the Neurological Status and Quality of Life of Patients with Herpesvirus Infection. / Rasulova R.P., Kuranbaeva S.R. // ISSN 2181-5534 Infection, Immunity and Pharmacology. Tashkent: No. 3/2022. 188-193. |
| [10] | Neurological characteristics of patients with Postherpetic trigeminal neuralgia. / Raykhon P. Rasulova, Satima R. Kuranbaeva // MedForum: International Conference on Patient-Centered Approaches to Medical Intervention 2024 ˗ Taylor & Francis Group, London. ˗ 35-37. |
| [11] | Prikhodchenko N. G. Infection Caused by Varicella-Zoster Virus: Features of the Course, Clinical Manifestations, Complications, and Prevention Possibilities // Therapeutic Archive. - 2021. ˗ Vol. 93. ˗ No. 11. ˗ P. 1401-1406. |
| [12] | Rasulova R.P., Bobojonov S.A., Xakimov U.R. Polish science journal International science journal. ISSUE 2(35) Part 3. Warsaw, Poland Wydawnictwo Naukowe "iScience" 2021: 222-225. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML