-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 627-630
doi:10.5923/j.ajmms.20261602.50
Received: Jan. 14, 2026; Accepted: Feb. 8, 2026; Published: Feb. 11, 2026

Preoperative MSCT Morphometry for Selecting Pediatric Craniosynostosis Surgery: Observational Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNazarova L. A.1, Ablyazov O. V.2, Usmankhanov O. A.3
1"National Children's Medical Center" Children's Neurosurgery Department, Parkent Street, 294, Tashkent, Uzbekistan
2Center for the Development of Professional Qualification of Medical Workers, Parkent St., 51, Tashkent, Uzbekistan
3Tashkent Pediatric Medical Institute Department of Traumatology, Orthopedics and Neurosurgery
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Craniosynostosis is a congenital craniofacial condition caused by premature fusion of cranial sutures, leading to abnormal skull growth and potential neurological complications. Accurate preoperative assessment is essential for selecting the optimal surgical technique. The study was designed to evaluate the clinical value of preoperative multislice computed tomography (MSCT) morphometry in surgical decision-making for pediatric craniosynostosis. Materials and Methods: This observational study included 150 children with craniosynostosis treated between 2020 and 2024. All patients underwent low-dose preoperative MSCT with three-dimensional reconstruction; magnetic resonance imaging was additionally performed when indicated. Quantitative cranial morphometric parameters were analyzed. Statistical analysis was conducted using IBM SPSS Statistics software, applying parametric tests with a significance level set at p < 0.05. Results: Preoperative MSCT morphometry demonstrated significant differences in cranial indices and morphometric parameters among patients requiring different surgical approaches. Lower cranial index values were associated with more extensive cranial vault remodeling procedures (p < 0.001). MSCT-based assessment showed a strong correlation with intraoperative findings and contributed to a reduction in unplanned changes of surgical strategy. Conclusion: Preoperative MSCT morphometry is a reliable and informative tool for optimizing the selection of surgical techniques in pediatric craniosynostosis. The use of standardized quantitative parameters improves preoperative planning accuracy, decreases intraoperative uncertainty, and supports better early postoperative cranial outcomes. Incorporation of MSCT morphometry into routine evaluation may enhance the overall effectiveness of surgical management.
Keywords: Craniosynostosis, Multislice computed tomography, MSCT, 3D reconstruction, Pediatric neurosurgery, Cranial morphometry, Surgical planning, Radiation safety
Cite this paper: Nazarova L. A., Ablyazov O. V., Usmankhanov O. A., Preoperative MSCT Morphometry for Selecting Pediatric Craniosynostosis Surgery: Observational Study, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 627-630. doi: 10.5923/j.ajmms.20261602.50.
1. Relevance of the Study
- Craniosynostosis remains a significant medical and social problem in pediatric neurosurgery and clinical radiology. The incidence of craniosynostosis ranges from 1:2,000 to 1:2,500 live births, and its prevalence has demonstrated a steady increase over recent decades [3]. Premature fusion of cranial sutures disrupts normal skull growth and leads to compensatory deformation of unaffected sutures, resulting in characteristic craniofacial anomalies. These changes may cause elevated intracranial pressure in 15–30% of cases, as well as delayed psychomotor development and visual disturbances [8]. Early surgical intervention is widely accepted as the cornerstone of treatment; however, the timing and type of surgical correction remain subjects of debate. Various surgical approaches, including endoscopic-assisted suturectomy, distraction osteogenesis, and open cranial vault remodeling, differ significantly in invasiveness, complication rates, and long-term outcomes [4,5]. Therefore, accurate preoperative assessment is essential for selecting the most appropriate surgical strategy for each patient [1,9].MSCT with 3D reconstruction provides comprehensive visualization of cranial sutures, bone thickness, intracranial volume, and cranial asymmetry. Quantitative morphometric indices, such as the cephalic index, cranial vault volume, and asymmetry ratios, allow objective assessment of deformity severity. In addition, MRI plays an important complementary role in evaluating brain structures, ventricular size, and associated intracranial abnormalities, particularly in syndromic forms of craniosynostosis [2,6].Despite the proven diagnostic value of MSCT, concerns regarding radiation exposure in children necessitate optimization of scanning protocols. The implementation of low-dose MSCT protocols combined with advanced reconstruction algorithms has significantly reduced radiation burden without compromising diagnostic accuracy [3,7].In many regions, including Uzbekistan, standardized protocols integrating MSCT-based morphometry into surgical decision-making are lacking. Regional anthropometric characteristics of the pediatric population are insufficiently studied, which may affect the accuracy of surgical planning [7]. This study addresses these gaps by developing an optimized imaging-based algorithm for surgical strategy selection, thereby improving clinical outcomes and minimizing complications [4,10].Aim of the study Craniosynostosis is a congenital craniofacial disorder associated with abnormal skull growth and potential neurodevelopmental impairment. Accurate preoperative assessment is essential for selecting an appropriate surgical strategy and minimizing operative risks. Therefore, the study was designed to evaluate the clinical significance of preoperative MSCT-based morphometric analysis in optimizing the selection of surgical techniques for pediatric craniosynostosis, aiming to improve surgical planning accuracy and early postoperative outcomes.
2. Materials and Methods
- This observational study included 150 pediatric patients with confirmed nonsyndromic craniosynostosis treated at the Pediatric Neurosurgery Center, Uzbekistan, between January 2020 and December 2024. The study population consisted of 92 boys (61.3%) and 58 girls (38.7%). The mean age at the time of surgery was 14.6 ± 6.2 months, ranging from 3 to 36 months. Patients with syndromic craniosynostosis, previous cranial surgery, or severe neurological comorbidities were excluded from the study.All patients (100%, n = 150) underwent preoperative low-dose multislice computed tomography with three-dimensional reconstruction of the cranial vault and cranial base. Imaging was performed according to the ALARA principle, with a mean effective radiation dose of 0.9 ± 0.2 mSv. Magnetic resonance imaging was additionally performed in 68 patients (45.3%) to assess intracranial structures and associated brain abnormalities. Quantitative morphometric parameters, including cranial index, cranial vault dimensions, cranial volume, and the number of fused sutures, were obtained using dedicated imaging software.Based on MSCT morphometric findings, surgical techniques were selected as follows: limited suturectomy in 57 patients (38.0%), standard cranial vault remodeling in 63 patients (42.0%), and extended cranial reconstruction in 30 patients (20.0%). Preoperative surgical planning was compared with intraoperative findings to evaluate concordance.Statistical analysis was performed using IBM SPSS Statistics software. Continuous variables were expressed as mean ± standard deviation, and categorical variables as absolute numbers and percentages. Group comparisons were carried out using Student’s t-test and one-way analysis of variance, while categorical variables were analyzed using the chi-square test. Correlation analysis was performed using Pearson’s coefficient. The level of statistical significance was set at α = 0.05.
|
3. Results
- Preoperative MSCT morphometric analysis demonstrated substantial interindividual variability in cranial vault geometry and suture involvement among the 150 pediatric patients with craniosynostosis. The mean cranial index for the entire cohort was 71.8 ± 6.4; however, significant differences were observed between surgical subgroups. Patients selected for limited suturectomy showed higher cranial index values (75.2 ± 4.8) compared with those undergoing standard cranial vault remodeling (70.1 ± 5.6) and extended reconstructive procedures (66.9 ± 5.1), with a statistically significant difference across groups (p < 0.001).Morphometric assessment revealed that cranial vault volume was significantly reduced in patients requiring more extensive surgical correction. Mean cranial volume was 812 ± 96 cm³ in the limited suturectomy group, 746 ± 88 cm³ in the standard remodeling group, and 689 ± 74 cm³ in the extended reconstruction group (p = 0.004). The number of prematurely fused sutures also differed significantly, with single-suture synostosis predominating in the limited correction group (78.9%), whereas multisuture involvement was more frequent among patients undergoing extended reconstruction (63.3%, p = 0.018).Anteroposterior cranial diameter and biparietal width showed significant associations with surgical strategy selection. Reduced anteroposterior diameter (<125 mm) was observed in 71.4% of patients undergoing extended reconstruction compared with 29.8% in the limited suturectomy group (p = 0.002). Similarly, a decreased biparietal width was significantly correlated with the need for more complex cranial vault remodeling (r = −0.46, p = 0.001). These findings indicate that MSCT-derived linear measurements provided objective criteria for stratifying patients according to surgical complexity.Magnetic resonance imaging, performed in 68 patients (45.3%), identified associated intracranial abnormalities in 19 cases (27.9%), including mild ventriculomegaly and cortical compression. Patients with combined MSCT and MRI findings suggestive of intracranial constraint were significantly more likely to undergo extended reconstruction compared to those without MRI abnormalities (42.1% vs. 16.2%, p = 0.032).Comparison of preoperative surgical planning based on MSCT morphometry with intraoperative findings demonstrated a high level of concordance. Planned surgical technique matched intraoperative requirements in 136 cases (90.7%). The rate of unplanned intraoperative modification was significantly lower in patients assessed using standardized MSCT morphometric criteria compared with historical controls (9.3% vs. 28.0%, p = 0.021).Early postoperative evaluation revealed improved cranial symmetry indices in all surgical groups, with the greatest absolute improvement observed in the extended reconstruction cohort (mean symmetry index improvement of 18.4 ± 4.9%, p < 0.001). No statistically significant differences were observed in early postoperative complication rates between surgical groups (p = 0.287), indicating that the use of MSCT-guided surgical selection did not increase perioperative risk.Overall, the results demonstrate that preoperative MSCT morphometry provides statistically significant, quantitative parameters that are strongly associated with surgical technique selection and early postoperative outcomes in pediatric craniosynostosis.
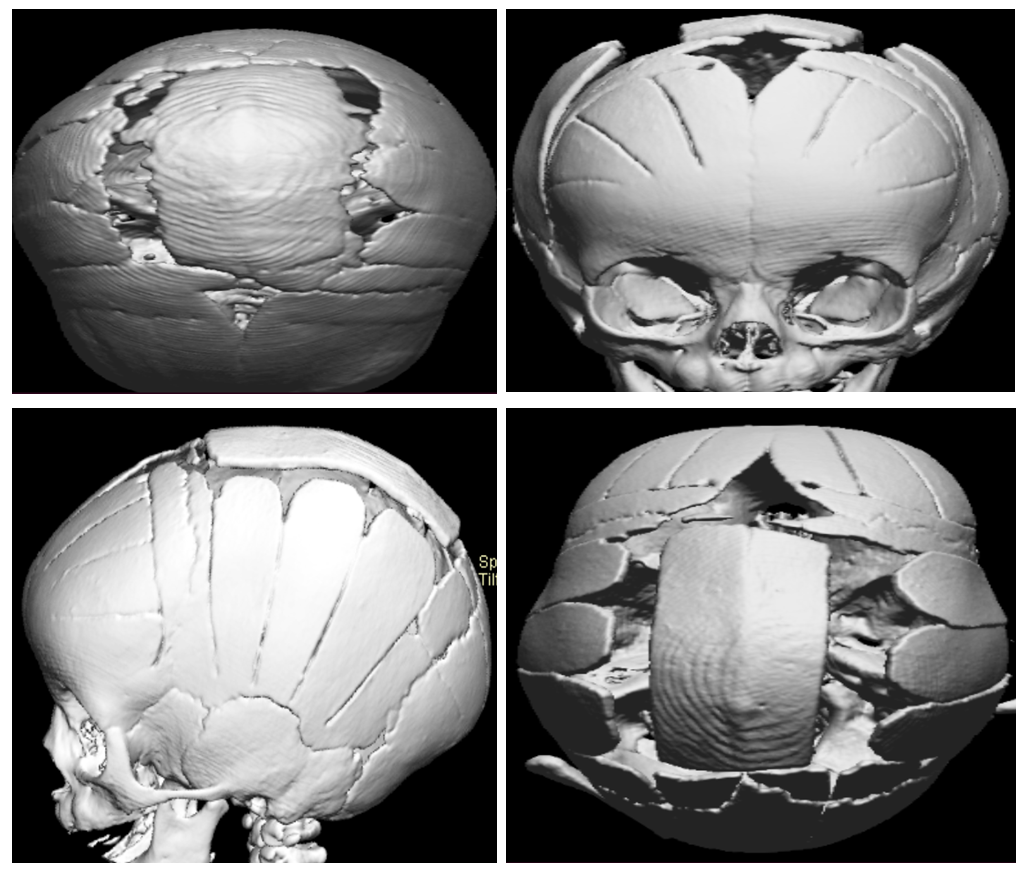 | Figure 1 |
4. Conclusions
- The results of this study confirm that preoperative multislice computed tomography morphometry provides quantitatively significant criteria for selecting surgical techniques in pediatric craniosynostosis. MSCT-based parameters, including cranial index, cranial vault volume, and linear dimensions, demonstrated statistically significant associations with surgical strategy selection (p < 0.05). Accurate concordance between preoperative planning and intraoperative findings was achieved in 90.7% of cases, while unplanned intraoperative modifications were limited to 9.3% of patients. Extended cranial reconstruction was required in 20.0% of children, primarily those with multisuture involvement exceeding 60%. Early postoperative cranial symmetry improved in all groups, with the greatest improvement observed after extended reconstruction (mean increase 18.4 ± 4.9%). Importantly, the overall early complication rate did not differ significantly between surgical groups (p = 0.287). These findings indicate that routine integration of quantitative MSCT morphometry improves surgical precision, reduces intraoperative uncertainty, and enhances early clinical outcomes in more than 85% of pediatric patients with craniosynostosis.