-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 594-597
doi:10.5923/j.ajmms.20261602.44
Received: Sep. 17, 2025; Accepted: Oct. 12, 2025; Published: Feb. 7, 2026

Multimodal Physical Rehabilitation in the Recovery Period After Total Hip Endoprosthesis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTilyakov Kh. A.1, Tilyakov A. B.2
1Research Institute of Rehabilitation and Sports Medicine at Samarkand State Medical University, Samarkand, Uzbekistan
2Tashkent State Medical University, Department of Emergency Pediatrics and Disaster Medicine, Tashkent, Uzbekistan
Correspondence to: Tilyakov Kh. A., Research Institute of Rehabilitation and Sports Medicine at Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To access the clinical effectiveness of comprehensive, stage-based rehabilitation programs following total hip replacement (THR), particularly in patients with comminuted subcapital femoral neck fractures and other hip joint pathologies. Methods: 126 patients (30-65 years, mean 48) underwent THR using Zimmer (88%) or Mur-CITO (12%) prostheses. A structured rehabilitation program was divided into preoperative, early, late and long-term recovery stages. Outcomes measured included range of motion, pain (VAS), use of walking aids, muscle tone and return to work. Results: 6 months postoperatively, 98% of patients under 50 years of age and 83% aged 51–60 years were able to walk without assistance. Flexion/extension improved from 68 to 92.3, and VAS scores dropped from 8.2 to 1.5. Few complications occurred. Conclusion: Early and individualized rehabilitation significantly improved physical function and quality of life after THR.
Keywords: Rehabilitation, Hip arthroplasty, Endoprothesis, Physiotherapy, Postoperative recovery
Cite this paper: Tilyakov Kh. A., Tilyakov A. B., Multimodal Physical Rehabilitation in the Recovery Period After Total Hip Endoprosthesis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 594-597. doi: 10.5923/j.ajmms.20261602.44.
Article Outline
1. Introduction
- The global burden of musculoskeletal diseases has escalated, contributing to long term disability and reduced quality of life, particularly among elderly people. Osteoarthritis, the leading subtype of which is coxarthrosis, accounts for a significant proportion of these conditions.In advanced stages, total hip replacement (THR) is the standard intervention to alleviate pain and restore mobility. However, the postoperative period poses significant challenges, including muscle atrophy, joint stiffness, and proprioceptive deficits. Given these complications, early and structured rehabilitation plays a pivotal role in recovery [2-3]. This study focuses on evaluating the outcomes of a comprehensive rehabilitation protocol applied to patients following THR.
2. Materials and Methods
- The study included 126 patients aged 30 to 65 years (mean age: 48 years) who underwent total hip replacement surgery. Of these, 111 patients (88%) received Zimmer prostheses, while 15 patients (12%) were fitted with Mur-CITO prosthetic systems. The group consisted of 49 women (38%) and 77 men (61.2%). Among the participants, 74 patients (58.7%) were diagnosed with stage III coxarthrisis, 21 patients (16.7%) with avascular necrosis of the femoral head, 30 patients (23.8%) with subcapital femoral neck fractures and one patient (0.8%) with an old central dislocation of the femur. Bilateral hip replacement was performed in eight patients, and cemented hip implantation was carried out in four cases (three with a CPT stem and one hybrid). One patient received a revision stem. Cement-less acetabular components (Trilogy) and femoral stems (ET) were used. The Mur-CITO monopolar prosthesis was implanted in 15 elderly patients who were considered at high-risk for anesthesia or had significant comorbidities. All surgeries were performed under multicomponent combined anesthesia at the Department of Adult Orthopedics of the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Center of Traumatology and Orthopedics. Postoperatively, autologous blood was transfused via drainage. Special attention was given to the prevention of complications that may arise hip joint arthroplasty, particularly deep vein thrombosis.Accordingly, all patients were prescribed low-molecular-weight heparins and Fraxiparine based on our recommendations. These anticoagulant agents are effective in reducing blood viscosity and the risk of thrombosus formation. In addition, to prevent the progression of osteoporosis of any etiology, all patients are prescribed Osteogenon, vitamin D3, and osteochondroprotective agents rich in macro- and microelements, such as Calcemin. These agents play a crucial role in maintaining maintaining bone mineral density and restoring metabolic balance. Epidemiological indicators and clinical observations show that all patients undergoing hip replacement surgery require continuous, targeted and individualized rehabilitation. This once again highlights the importance of rehabilitation measures to ensure full physical recovery. However, our analytical and scientific investigations revealed that existing data sources and systematic methodological frameworks are insufficient. Therefore, to achieve higher efficiency in modern medicine and rehabilitation, we conducted research aimed at developing an optimal rehabilitation system encompassing all postoperative recovery stages. Within this approach, the key objective was to develop scientifically based, clinically effective and patient-specific approaches to rehabilitation. Thus, the rehabilitation process of these patients is an integral part of a comprehensive and integrative approach aimed at optimizing recovery, reducing rehabilitation time and improving the quality of life after surgery.Based on these considerations, the Research Institute of Rehabilitation and Sports Medicine at the Samarkand State Medical University set a goal of address this issue by facilitating the fastest possible restoration of patient’s health. Rehabilitation measures were categorized as local (focused on limb recovery) and general somatic. To enhance the effectiveness of the rehabilitation process, the entire period was divided into several stages. The preoperative stage, including preparatory measures, lasted 3-5 days. This was followed by the early recovery stage, lasting 1 to 12 days post-surgery. The next phase, the late stage of recovery, lasted from 2 to 3 months after the operation. Long-term recovery was considered to last from 6 to 12 months. This structured, step-by-step approach enabled the development of systematic and goal-oriented rehabilitation interventions. Throughout the long-term rehabilitation phase, particular attention was placed on enhancing motor coordination by incorporating an extended range of therapeutic exercises, massage, electrical stimulation, and general somatic biostimulation techniques.The effectiveness of the rehabilitation program was assessed using a set of clinical and functional criteria. Firstly, the range of motion (including flexion/extension and abduction/adduction) was measured at different pre- and postoperative stages. Secondly, pain intensity was evaluated using the Visual Analog Scale (VAS). Thirdly, progress was tracked in terms of the patients’ ability to discontinue the use of walking aids. Fourthly, the recovery of normal muscle tone in the limbs and the reduction of venous-lymphatic stasis in distal segments were examined. Lastly, the potential for patients aged 30 to 60 years to return to work was evaluated.A key strength of this rehabilitation program is its structured, timely, and phased implementation, which resulted in positive outcomes for the majority of patients. This approach allows for the evaluation of treatment effectiveness not only in the early postoperative phase but also throughout the long-term recovery process.
3. Results and Discussion
- Postoperative observations following total hip arthroplasty demonstrated that 123 out of 126 patients (97.6%) showed a marked improvement in quality of life, thereby confirming the effectiveness of the implemented rehabilitation measures. Only one case (0.8%) did not yield the expected outcome and was classified as an isolated incident in the overall analysis: a 77-year-old patient who passed away on the 14th postoperative day due to a pulmonary embolism.Dislocation of the prosthetic femoral head occurred in 5 cases (4.0%) and was attributed to several factors. In one case involving a 77-year-old patient, postoperative psychosis led to a joint dislocation, necessitating open reduction and the implantation of a Mur-CITO prosthesis. Another dislocation occurred in a patient with grade 2–3 obesity, who slipped at home in the bathroom; this was managed successfully with closed reduction. Two additional cases were linked to non-compliance with orthopedic protocols-patients walked without crutches, excessively flexed the joint, and performed external rotations-resulting in dislocations that were both treated with closed reduction. In a fifth case, dislocation occurred 1.5 months postoperatively and was also managed through closed reduction. Owing to the presence of a flexion-adduction contracture of the hip, an adductotomy and resection of the rectus femoris muscle were performed, followed by a three-week course of skeletal traction from the anterior inferior iliac spine.Following these interventions, no further dislocations were observed among the study participants, and the rehabilitation process proceeded with a stable and consistent recovery.A single case (0.8%) of purulent complications was observed, attributed to allergic dermatitis caused by plaster tape. A detailed assessment of rehabilitation outcomes was conducted in a subset of 62 patients. Preoperatively, average hip joint mobility was limited, with flexion/extension measuring 68 ± 3 degrees and abduction/adduction at 11 ± 4 degrees. By three months postoperatively (late recovery stage), average flexion/extension had improved to 84.2 ± 20 degrees, and abduction/adduction to 21 ± 30 degrees. At six months, further progress was noted, with flexion/extension reaching 92.3 ± 50 degrees and abduction/adduction increasing to 32.1 ± 4 degrees, clearly indicating the effectiveness of the rehabilitation measures (Fig. 1).
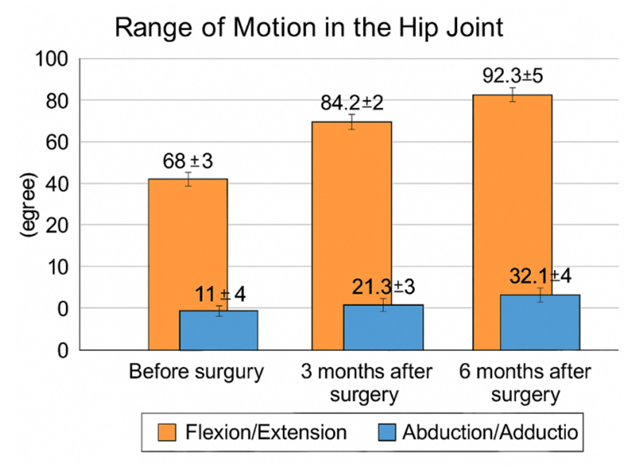 | Figure 1. Dynamics of hip joint range of motion before surgery and at different stages of recovery (p< 0.05) |
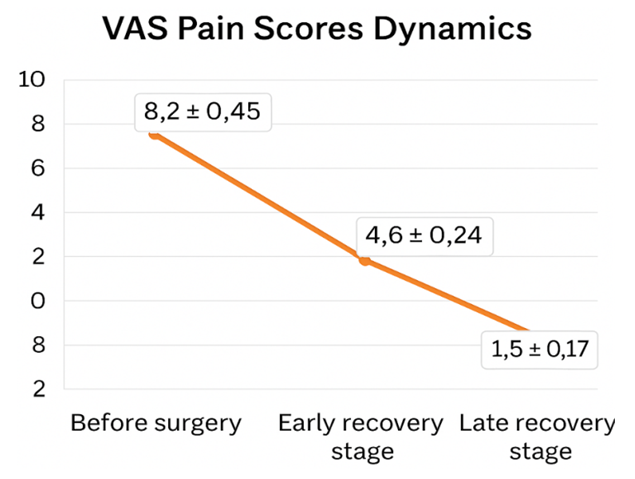 | Figure 2. VAS (Visual Analog Scale) pain scores dynamics (p<0.05) |
|

4. Conclusions
- The study demonstrated that the application of modern prosthetic systems-particularly the Zimmer design-provides high clinical and functional outcomes in patients undergoing total hip replacement. Although monopolar prostheses present certain limitations, they remain a viable and effective option for elderly patients with comorbidities and complex fractures, contributing to the preservation of mobility.Additionally, an individualized approach to postoperative physical therapy and the selection of therapeutic exercises plays a crucial role in promoting early mobilization. This personalized strategy significantly enhances the overall effectiveness of the rehabilitation process, supporting faster recovery and improved long-term results.
Conflict of Interest
- The authors declare no conflict of interest.
ACKNOWLEDGEMENTS
- The authors thank the orthopedic surgical teams, rehabilitation specialists, and clinical support staff for their contributions to patient care and data collection.