-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 588-593
doi:10.5923/j.ajmms.20261602.43
Received: Jan. 7, 2026; Accepted: Jan. 25, 2026; Published: Feb. 7, 2026

Clinical and Biochemical Phenotyping of Children with Congenital Heart Disease and Pulmonary Hypertension Before and After Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAshurova D. T., Turaeva Y. Sh.
Department of Propaedeutics of Childhood Disease, Tashkent State Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Pulmonary hypertension (PH) is a major modifier of perioperative risk in children with congenital heart disease (CHD) and is associated with increased susceptibility to early postoperative complications [3,4]. Oxidative stress has been implicated as a key mechanism underlying postoperative vulnerability; however, data on perioperative antioxidant dynamics in pediatric CHD patients with PH remain limited [5,7,8,9]. Objective: To evaluate perioperative changes in oxidative stress markers—superoxide dismutase (SOD) activity and total antioxidant status (TAS)—in children with congenital heart disease with and without pulmonary hypertension undergoing surgical correction. Methods: This observational study included children with CHD stratified according to the presence of pulmonary hypertension. Oxidative stress markers were assessed preoperatively (T0) and in the early postoperative period (T1). Superoxide dismutase activity and total antioxidant status were measured using spectrophotometric methods. Clinical postoperative course parameters were analyzed in parallel. Data are presented as mean ± standard deviation, and intergroup comparisons were performed using appropriate statistical tests. Results: Children with pulmonary hypertension demonstrated significantly lower preoperative SOD activity compared with patients without pulmonary hypertension. In the early postoperative period, SOD activity increased modestly in both groups but remained significantly lower in children with PH. Total antioxidant status showed a similar trend, with reduced baseline values and incomplete postoperative recovery in the PH group. These findings indicate persistent impairment of antioxidant defense mechanisms in children with CHD complicated by pulmonary hypertension. Conclusion: Children with congenital heart disease and pulmonary hypertension exhibit sustained perioperative oxidative stress characterized by reduced antioxidant capacity. Assessment of SOD activity and total antioxidant status provides valuable insight into biological vulnerability and may contribute to improved perioperative risk stratification and individualized postoperative management in pediatric cardiac surgery.
Keywords: Congenital heart disease, Pulmonary hypertension, Oxidative stress, Superoxide dismutase, Total antioxidant status, Pediatric cardiac surgery
Cite this paper: Ashurova D. T., Turaeva Y. Sh., Clinical and Biochemical Phenotyping of Children with Congenital Heart Disease and Pulmonary Hypertension Before and After Surgery, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 588-593. doi: 10.5923/j.ajmms.20261602.43.
1. Introduction
- Congenital heart disease (CHD) remains the most common group of congenital anomalies in childhood and continues to be a leading cause of morbidity and mortality despite significant advances in pediatric cardiac surgery [1,2]. Among children with CHD, the presence of pulmonary hypertension (PH) represents a particularly unfavorable clinical condition that substantially complicates perioperative management and adversely affects early postoperative outcomes [3,4].Pulmonary hypertension in CHD is associated not only with altered pulmonary hemodynamics but also with systemic pathophysiological changes, including endothelial dysfunction, chronic hypoxia, oxidative stress, and immune dysregulation [3,4,10]. These mechanisms increase the vulnerability of pediatric patients to cardiopulmonary bypass–related stress and contribute to the development of postoperative respiratory and infectious complications.Oxidative stress plays a central role in myocardial and pulmonary injury during surgical correction of CHD [5,6,7,9,11]. An imbalance between pro-oxidant activity and antioxidant defense systems may limit adaptive responses to surgical stress, particularly in children with PH. Total antioxidant status (TAS) and superoxide dismutase (SOD) have been proposed as integral markers reflecting the functional reserve of the antioxidant system and the capacity to neutralize reactive oxygen species in the perioperative period [6,7,11,12].In parallel, alterations in humoral and cellular immunity have been increasingly recognized as important contributors to postoperative vulnerability in pediatric cardiac patients [10,12]. Changes in immunoglobulin levels and lymphocyte subpopulations may reflect both chronic disease burden and acute immunological stress induced by surgery, thereby influencing susceptibility to early infectious and inflammatory complications.Despite growing evidence addressing individual biochemical or immunological abnormalities in children with CHD, data integrating clinical, laboratory, immunological, and instrumental parameters into a unified phenotypic framework remain limited. In particular, comparative phenotyping of children with and without PH before and after surgical intervention has not been sufficiently explored.The aim of the present study was to perform a comprehensive clinical and biochemical phenotyping of children with congenital heart disease and pulmonary hypertension before and after surgical correction, focusing on oxidative stress markers, immune status, routine laboratory parameters, echocardiographic characteristics, and early postoperative complications.
2. Materials and Methods
- This observational study included children with congenital heart disease who underwent surgical correction in a specialized pediatric cardiac surgery setting. Patients were stratified into two groups according to the presence or absence of pulmonary hypertension, as determined by echocardiographic criteria. Clinical, laboratory and instrumental evaluations were conducted in the preoperative period and repeated in the early postoperative phase. Routine clinical assessment included demographic characteristics, duration of respiratory support, length of intensive care unit stay and total hospital stay. Laboratory investigations encompassed complete blood count and standard biochemical blood analysis, including parameters reflecting metabolic and protein status.Oxidative stress was assessed by measuring total antioxidant status and superoxide dismutase activity before and after surgery. Immune status evaluation comprised humoral immunity markers, including immunoglobulin G, A and M, as well as cellular immunity parameters represented by lymphocyte subpopulations expressing CD3, CD4, CD8, CD20 and CD38 antigens. Echocardiographic examination was performed to assess left ventricular end-diastolic volume, characteristics of septal defects when present, and pulmonary artery pressure. Postoperative chest radiography was used to identify respiratory complications such as pneumonia and bronchitis.Statistical analysis was performed using appropriate parametric or non-parametric methods depending on data distribution, with intergroup comparisons, intra-group dynamics and correlation analyses applied as indicated. Statistical significance was defined as a p-value of less than 0.05. The integrated assessment of clinical, biochemical, immunological and instrumental parameters was undertaken to characterize phenotypic differences between children with congenital heart disease with and without pulmonary hypertension and to evaluate their evolution in the early postoperative period.
3. Results
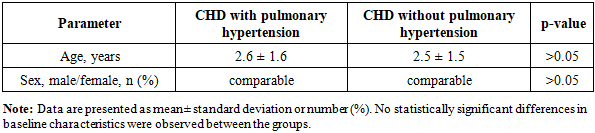
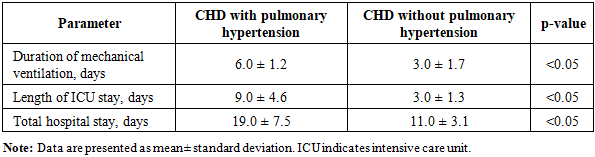
- The study included children with congenital heart disease stratified according to the presence of pulmonary hypertension. The mean age of the study population was 2.6 ± 1.6 years, with no statistically significant age difference between the groups (Table 1). Clinical course in the early postoperative period differed markedly between patients with and without pulmonary hypertension. Children with pulmonary hypertension required significantly longer duration of mechanical ventilation, with a mean of 6.0 ± 1.2 days, compared to 3.0 ± 1.7 days in patients without pulmonary hypertension (p < 0.05). Similarly, the length of stay in the intensive care unit was prolonged in the pulmonary hypertension group (9.0 ± 4.6 days versus 3.0 ± 1.3 days), as was total hospital stay (19.0 ± 7.5 days versus 11.0 ± 3.1 days), indicating a more severe and prolonged postoperative course (Table 2).
|
|
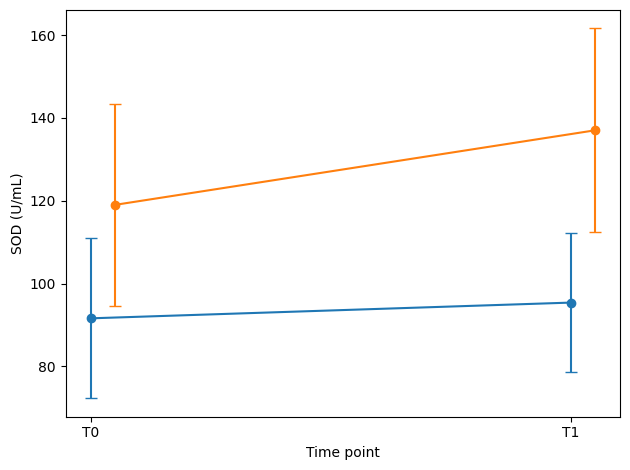 | Figure 1. Perioperative dynamics of superoxide dismutase activity in children with congenital heart disease |
|
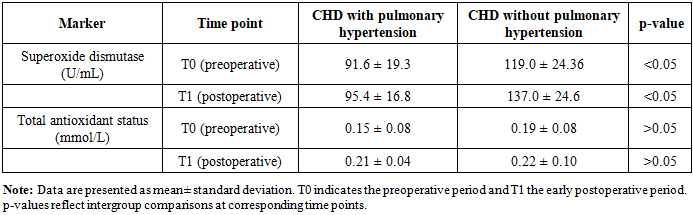
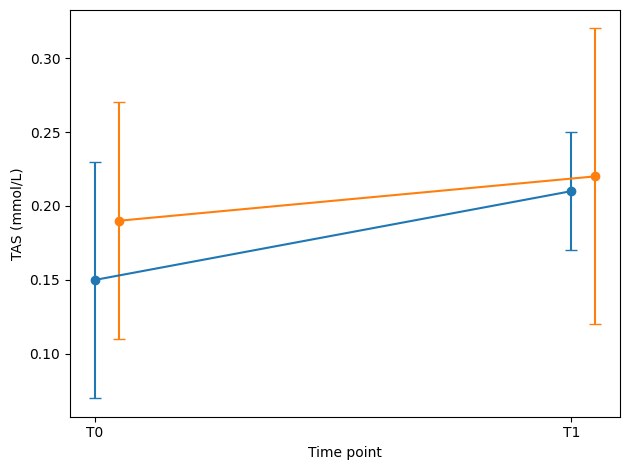 | Figure 2. Perioperative dynamics of oxidative stress markers in children with congenital heart disease |
|
|
|
4. Discussion
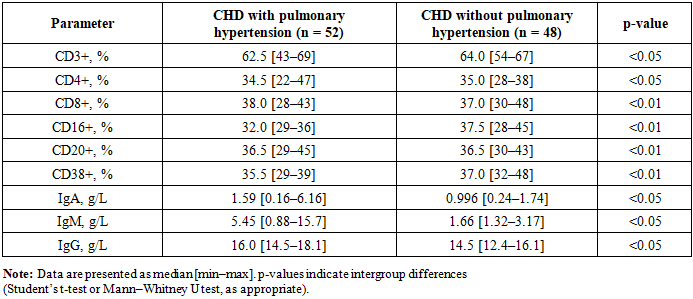
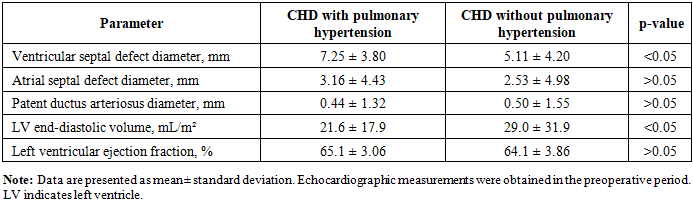
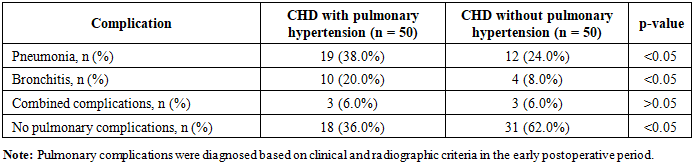
- The results of the present study demonstrate that children with congenital heart disease and pulmonary hypertension represent a distinct clinical and biological phenotype characterized by increased postoperative vulnerability, persistent oxidative stress imbalance and immune system dysregulation. The integration of clinical parameters, laboratory findings and instrumental data revealed that the unfavorable postoperative course observed in this group cannot be explained solely by anatomical or surgical factors, but rather reflects complex systemic pathophysiological mechanisms.One of the most prominent findings of this study was the pronounced impairment of antioxidant defense in children with pulmonary hypertension, as evidenced by significantly lower baseline superoxide dismutase activity and total antioxidant status prior to surgical intervention. These abnormalities persisted in the early postoperative period despite partial recovery of antioxidant markers, indicating a limited adaptive reserve in response to surgical stress. The incomplete normalization of oxidative stress parameters after surgery suggests that pulmonary hypertension is associated with chronic redox imbalance, which may exacerbate tissue injury during cardiopulmonary bypass and impair postoperative recovery. Similar observations have been reported in previous pediatric studies, highlighting the contribution of oxidative stress to myocardial and pulmonary dysfunction following cardiac surgery [5,6,7,9,11].The association between reduced antioxidant capacity and prolonged mechanical ventilation, extended intensive care unit stay and longer hospitalization observed in the pulmonary hypertension group further supports the clinical relevance of oxidative stress phenotyping [8,11]. The correlations identified between pulmonary artery pressure and superoxide dismutase activity indicate an interaction between hemodynamic burden and redox homeostasis, suggesting that elevated pulmonary vascular resistance may amplify oxidative stress responses and limit postoperative adaptation.In parallel with redox disturbances, children with pulmonary hypertension exhibited marked alterations in humoral and cellular immunity. Lower preoperative immunoglobulin concentrations likely reflect chronic immune system strain associated with prolonged hypoxia and systemic inflammation. Postoperatively, incomplete recovery of immunoglobulin levels and increased expression of immune activation markers, such as CD38-positive lymphocytes, indicate sustained immunological stress following surgical correction. These findings are consistent with the concept that pediatric patients with pulmonary hypertension enter surgery with pre-existing immune vulnerability, which may predispose them to postoperative infectious and inflammatory complications [10,12].The higher incidence of respiratory complications, including pneumonia and bronchitis, in children with pulmonary hypertension further underscores the clinical significance of combined oxidative and immune dysfunction [3,8,12]. Impaired antioxidant defense and altered immune responses may compromise pulmonary host defenses, thereby increasing susceptibility to postoperative respiratory pathology. The observed associations between biochemical phenotypes and radiographic findings suggest that early identification of high-risk patients based on laboratory markers could facilitate targeted postoperative monitoring and preventive strategies.Echocardiographic data confirmed that children with pulmonary hypertension exhibit more severe preoperative hemodynamic alterations, which only partially normalize after surgical correction. The persistence of elevated pulmonary artery pressure and altered ventricular parameters in the early postoperative period highlights the importance of considering pulmonary vascular pathology when interpreting postoperative outcomes. The interplay between hemodynamic stress, oxidative imbalance and immune dysregulation supports the concept of pulmonary hypertension as a systemic modifier of surgical risk rather than an isolated hemodynamic condition.Taken together, these findings emphasize the value of an integrated phenotypic approach in children with congenital heart disease. The combined assessment of oxidative stress markers, immune parameters and clinical indicators allows for more comprehensive characterization of postoperative vulnerability than routine evaluation alone. Such phenotyping may contribute to improved risk stratification, early identification of patients at increased risk of complications and optimization of perioperative management strategies in pediatric cardiac surgery.
5. Conclusions
- Сhildren with congenital heart disease and pulmonary hypertension constitute a distinct clinical and biological phenotype characterized by impaired antioxidant defense, immune system dysregulation and a more severe early postoperative course. Reduced preoperative levels of total antioxidant status and superoxide dismutase activity reflect limited adaptive reserve and persist partially after surgical correction. Alterations in humoral and cellular immunity further contribute to postoperative vulnerability and are associated with an increased incidence of respiratory complications. Echocardiographic evidence of sustained pulmonary hemodynamic burden underscores the systemic impact of pulmonary hypertension beyond isolated cardiovascular parameters. The integrated assessment of clinical, biochemical and immunological markers provides valuable insight into postoperative risk stratification. Incorporation of phenotypic profiling into routine perioperative evaluation may facilitate individualized management strategies and improve early outcomes in children undergoing surgery for congenital heart disease.