-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 567-571
doi:10.5923/j.ajmms.20261602.38
Received: Jan. 20, 2026; Accepted: Feb. 3, 2026; Published: Feb. 6, 2026

Results of the Evaluation of the Work on the Prevention of Bleeding in a Number of Obstetric Institutions in the Samarkand Region
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRizaev Jasur Alimjanovich1, Kattakhodjayeva Makhmuda Khamdamovna1, Abdullaeva Lola Saifullaevna2
1Doctor of Medical Sciences, Professor, Uzbekistan
2PhD, Samarkand State Medical University, Tashkent State Stomatological Institute, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Despite improvements in the quality of medical care worldwide, maternal mortality (MM) claims up to 300,000 women's lives every year. According to statistics, the risk of maternal mortality in developing countries is 100 times higher than in Europe [2,3]. The leading cause of MD today is still obstetric hemorrhage. The risk of hemorrhage among pregnant women exists from the early stages of pregnancy and throughout its duration. Postpartum hemorrhage, accompanied by massive blood loss, hemorrhagic shock, and multiple organ failure, causes particularly serious damage to women's health and even their lives [4].
Keywords: Hemorrhage, Massive blood loss, Pregnancy, Maternal mortality
Cite this paper: Rizaev Jasur Alimjanovich, Kattakhodjayeva Makhmuda Khamdamovna, Abdullaeva Lola Saifullaevna, Results of the Evaluation of the Work on the Prevention of Bleeding in a Number of Obstetric Institutions in the Samarkand Region, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 567-571. doi: 10.5923/j.ajmms.20261602.38.
Article Outline
1. Introduction
- About 80% of cases of obstetric hemorrhage lead to the development of a number of complications that damage a woman's health and, in some cases, accompany her for the rest of her life. Bleeding occurs more often in the first and third trimesters of pregnancy and can be triggered by a variety of factors that pose a threat to the mother and fetus. In some situations, there are no other pathological signs. About 25% of maternal deaths occur as a result of obstetric hemorrhages in the postpartum period [5]. At the same time, it should be noted that the number of maternal deaths is trending downward; over the past 30 years, Uzbekistan has seen a threefold decrease in maternal mortality. However, this indicator is still high compared to developed countries and in recent years has been 18-20 per 100,000 live births [6]. This raises the logical question: why, despite significant improvements in the material and technical base of medical institutions, the existence of national and local standards and protocols, and the improvement of the qualifications of medical workers, do the rates of hemorrhage and maternal mortality remain high, and what additional organizational measures are needed to improve the quality of medical care? In light of the above, we have attempted to analyze the quality of medical care for pregnant women at various levels of obstetric services. In order to assess the quality of medical care in regional maternity complexes and perinatal centers for the prevention of maternal mortality among pregnant women, an analysis of the activities of these institutions was conducted. To assess quality, questionnaires developed by the WHO as a tool for assessing and improving the quality of medical care for women to reduce preventable maternal and neonatal mortality were used, adapted to the conditions of Uzbekistan. Materials and methods. According to WHO recommendations, the assessment of the organization and quality of medical care is conducted anonymously. We conducted an assessment in six institutions—three obstetric complexes of central district hospitals, two city maternity hospitals, and an obstetric center (three levels of obstetric care)—evaluating the infrastructure of the institution, staffing, availability of essential medicines, necessary equipment, and consumables. The quality of care provided to pregnant women, women in labor, and women after childbirth was assessed by observing the organization of work on the prevention of bleeding during the provision of medical care. Attention was paid to the quality of the staff's work, the control of their work, the availability of care at night, its continuity, and the observance of patients' rights. Next, an analysis was conducted of medical record keeping and the availability of orders, guidelines, protocols, and the quality of their application. The quality assessment was conducted using a 3-point system, where 0 - extremely low quality care, serious risks to patient health identified. The institution needs significant improvement.1 - inadequate level of care, risks to patient health. Significant improvements are required. 2 - insufficient level of care, but no significant risk to patient health. Some improvements are necessary. 3 - care is provided in accordance with international standards. No improvement is required or only minimal changes are necessary.
2. Results and Discussion
- The results of the assessment of the facilities of the institutions studied showed that OPCs and some urban maternity hospitals had an appropriate structure and well-trained staff (22% of institutions), the remaining facilities had satisfactory infrastructure and were completely understaffed (11%), but most district-level maternity care facilities were in poor condition and in need of improvement (67%). An analysis of medical records showed that only 11% were fully compliant with standards, 56% had deficiencies in their completion, and 33% were poorly completed, Fig. 1. During diagnostic tests and treatment, filling out the partogram, and preventing bleeding, there were some deviations from the standards and protocols. There were cases of non-compliance with the sequence of certain procedures, technical errors in the completion of medical documentation, careless completion, and sometimes illegibility due to poor handwriting by doctors.
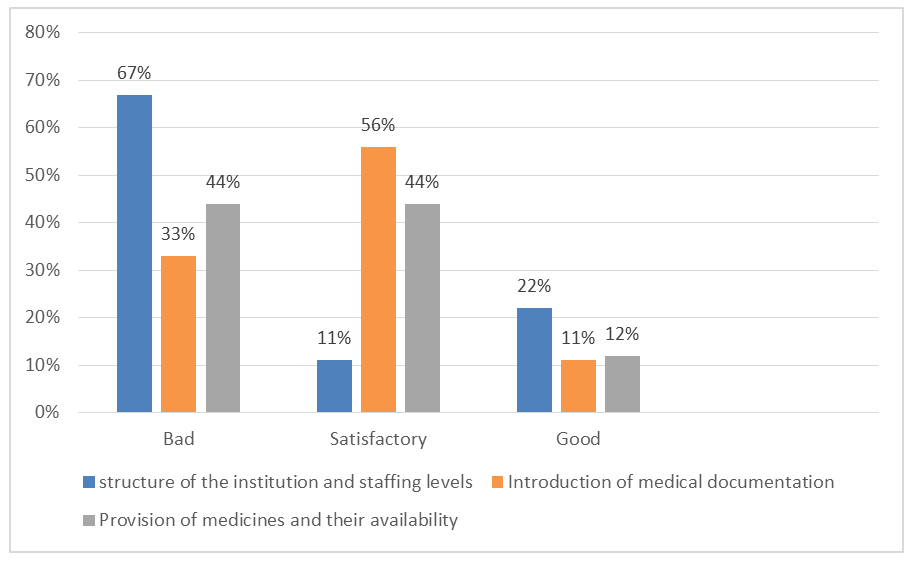 | Figure 1. Results of the study of the quality of work organization in obstetric care facilities at three levels |
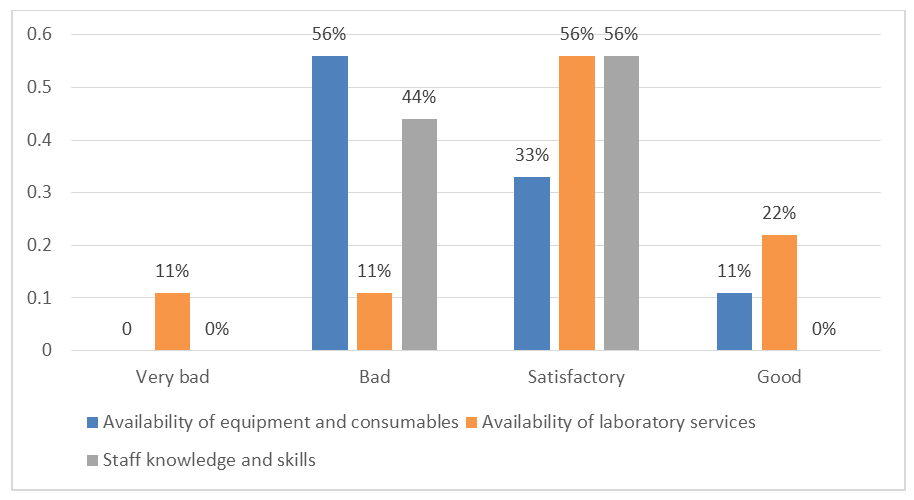 | Figure 2. Assessment of quality criteria for maternity care facilities |
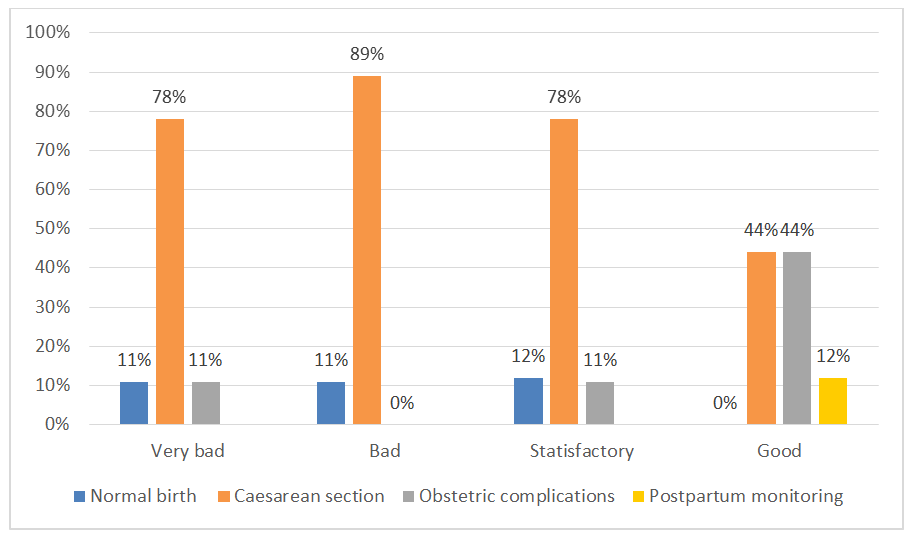 | Figure 3. Assessment of quality criteria in delivery rooms |
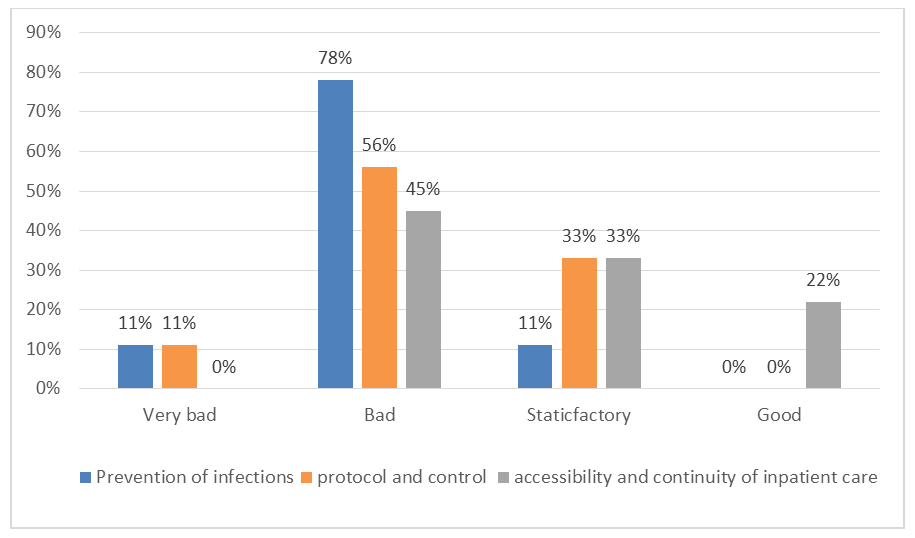 | Figure 4. Assessment of quality criteria in delivery rooms |
3. Conclusions for Improving the Work of Obstetricians - Gynecologists
- - Introduce practices to reduce the number of cesarean sections, perform surgery after 39 weeks and only when strictly indicated. - Conduct regular training of personnel on national protocols, explaining the importance of their implementation, and monitor their implementation at the hospital level;- Introduce adequate diagnostic criteria for massive bleeding and algorithms for managing obstetric hemorrhage;- Develop new protocols based on the principles of evidence-based medicine;- Use proven methods to improve the quality of medical services.
4. Recommendations for Maternity Facility Managers on the Prevention of Obstetric Hemorrhage
- - continue to develop and revise clinical protocols for the prevention and treatment of obstetric hemorrhage;- develop and implement algorithms and techniques for teamwork in cases of hemorrhage (organizing training in simulated situations) with regular monitoring;- bring infrastructure, laboratory equipment, and the supply of medicines and consumables into line with the requirements for the regionalization of obstetric care, ensure round-the-clock access, and strengthen the work of laboratory services; - Conduct ongoing training for all hospital staff using training sessions on combating obstetric hemorrhages in simulated conditions;- Create multidisciplinary teams in each institution (obstetricians-gynecologists, neonatologists, anesthesiologists, midwives, and nurses) to improve mutual understanding among staff within the institution and to standardize information for different institutions.