-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 563-566
doi:10.5923/j.ajmms.20261602.37
Received: Jan. 11, 2026; Accepted: Jan. 27, 2026; Published: Feb. 6, 2026

Electroencephalographic Correlates and Clinical Outcomes in Patients with Brain Tumors Undergoing Neurosurgical Intervention
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSharopov Sadullo Shukurilloyevich1, Khaydarov Nodirjon Kadirovich2
1Assistant at the Alfraganus University, Uzbekistan
2Professor at the Tashkent Medical University, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Brain tumors remain one of the most challenging neurological conditions, often accompanied by significant functional impairment and postoperative complications. Electroencephalography (EEG) provides direct insight into cortical activity, reflecting both local tumor effects and generalized brain dysfunction. Objective: To analyze the relationship between tumor localization, pathomorphological features, and postoperative neurological outcomes in patients with brain tumors, complemented by EEG correlates before and after neurosurgical intervention. Methods: Clinical and instrumental data from 100 patients aged 19–67 years (mean 43.3 ± 1.27 years) undergoing neurosurgical tumor removal from 2023 to 2025 were retrospectively analyzed. EEG patterns included frontal slow waves, epileptiform discharges, theta–delta oscillations, asymmetry of alpha rhythm, reduced visual alpha reactivity, photoparoxysmal responses, lateralized changes, and generalized slowing. Patients were stratified into two groups depending on localization and type of tumor. Results: Preoperative EEG indicated increased slow-wave activity (0.21±0.04 / 0.30±0.04), epileptiform discharges (0.15±0.03 / 0.20±0.04), and impaired alpha reactivity (0.01±0.01 / 0) with group-specific variations. Post-intervention data (under evaluation) are expected to demonstrate reduced epileptiform patterns and partial recovery of alpha responses, correlating with improved neurological status. Early findings suggest a relationship between tumor localization and lateralized EEG alterations, with pathomorphological types influencing the degree of postoperative complication risk. Conclusion: EEG serves as a valuable adjunctive tool for evaluating functional cortical states in brain tumor patients before and after surgery. Monitoring electrophysiological dynamics provides prognostic significance for anticipating neurological complications and guiding postoperative care.
Keywords: Brain tumors, Electroencephalography, Neurosurgery, Postoperative complications, Alpha rhythm, Slow waves
Cite this paper: Sharopov Sadullo Shukurilloyevich, Khaydarov Nodirjon Kadirovich, Electroencephalographic Correlates and Clinical Outcomes in Patients with Brain Tumors Undergoing Neurosurgical Intervention, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 563-566. doi: 10.5923/j.ajmms.20261602.37.
1. Introduction
- Brain tumors continue to represent one of the most significant challenges in modern neurology and neurosurgery, both for their complex biological behavior and their clinical implications. Despite advances in neuroimaging and surgical techniques, the morbidity and mortality associated with intracranial tumors remain high, particularly when diagnosis is delayed or when tumors are located in functionally critical brain regions (Ostrom et al., 2022) [1]. Accurate diagnostic methods that provide not only structural but also functional insights are therefore of considerable importance.Electroencephalography (EEG) is a well-established, non-invasive neurophysiological method that allows real-time evaluation of electrical brain activity. While magnetic resonance imaging (MRI) and histopathology remain the gold standards for diagnosis, EEG can reveal subtle functional disturbances that frequently precede clinical manifestations or structural progression (Stefan & Lopes da Silva, 2020) [2]. In particular, alterations in cortical rhythms such as alpha desynchronization, theta–delta predominance, focal slowing, and epileptiform discharges are often observed in brain tumor patients, reflecting disruption of thalamocortical connectivity and cortical irritability (Hughes & Rees, 2021) [3].Importantly, tumor-related EEG abnormalities do not occur in isolation, but rather correlate strongly with the localization, histological type, and growth dynamics of the tumor. For instance, slow-wave activity and focal epileptiform discharges are commonly associated with supratentorial masses, while reduced alpha reactivity and photoparoxysmal responses may be seen in patients with occipital and parietal tumors (Müller et al., 2020) [4]. Beyond diagnostic value, EEG patterns can predict perioperative risks: patients with preoperative epileptiform discharges may be predisposed to seizures following neurosurgical intervention, while generalized slowing may indicate diffuse cerebral dysfunction and reflect higher risk of complications (Shah et al., 2022) [5].Adolescents and adults in the pre-conscription and working-age categories are of particular interest, as preservation of neurological and visual-cognitive function in these patients has both medical and socio-economic relevance. Early identification of electrophysiological abnormalities may assist in guiding surgical planning, anticipate functional risks, and personalize rehabilitation strategies.Previous studies have often examined EEG in epilepsy or other neurodegenerative conditions, while systematic analysis of EEG correlates in brain tumor patients in Central Asia, particularly in Uzbekistan, remains limited. Moreover, few investigations have directly compared pre- and postoperative EEG dynamics in relation to morphological characteristics and clinical outcomes. This creates a clear research gap requiring multidimensional evaluation.The present study, therefore, aimed to analyze the clinical, morphological, and EEG data of 100 patients with brain tumors who underwent neurosurgical treatment between 2023 and 2025. Specific emphasis was placed on correlating tumor localization and histopathological type with baseline EEG abnormalities and postoperative neurological complications, thereby highlighting the prognostic potential of electrophysiological monitoring in brain tumor management.
2. Methods
- This study was conducted as a retrospective and partially prospective observational analysis of 100 patients with intracranial tumors who underwent neurosurgical treatment between 2023 and 2025. The study population included adult patients aged 19 to 67 years, with a mean age of 43.3 ± 1.27 years; 51 were male (51%, mean age 43.4 ± 1.83) and 49 female (49%, mean age 43.3 ± 1.80). All patients were admitted with suspected brain tumors confirmed by magnetic resonance imaging (MRI), followed by histopathological verification of tumor type according to the WHO 2021 classification. Exclusion criteria included a prior history of epilepsy not attributable to tumor, craniocerebral trauma, or severe systemic decompensated diseases that could confound EEG analysis. Patient selection and data processing were performed in accordance with ethical standards and approved by the institutional review board.Electroencephalography (EEG) was carried out in all patients preoperatively and in the early postoperative period (7–10 days after surgery). A standard 19-electrode montage was applied according to the international 10–20 system, with a sampling rate of 256 Hz and notch filtering at 50 Hz. Both eyes-open and eyes-closed resting conditions were recorded, in addition to intermittent photic stimulation to assess visual alpha reactivity and the presence of photoparoxysmal responses. Duration of each recording averaged 20 minutes, and analysis included both visual expert assessment and quantitative spectral analysis. The examined EEG variables comprised frontal slow waves, epileptiform discharges and speech artifacts, theta–delta waves with quasi-periodic complexes, asymmetry of the alpha rhythm with focal slowings or spikes, suppression of alpha reactivity to eye opening and photic stimulation, lateralized alterations without paroxysmal complexes, and overall diffuse slowing with reduced cortical reactivity. Quantitative indices were extracted and expressed as mean ± standard error of the mean (SEM), enabling between-group comparison.Patients were stratified into two analytical groups based on tumor localization and morphological type: Group 1 included patients with supratentorial tumors located predominantly in frontal and parietal regions, while Group 2 consisted of cases with deep-seated or temporo-occipital tumors. The rationale for this grouping was derived from the hypothesis that cortical and subcortical tumor localization exerts differential electrophysiological influences on background rhythms and seizure susceptibility. Surgical access, resection techniques, and perioperative management were standardized as per institutional neurosurgical protocols, thereby minimizing potential bias regarding treatment heterogeneity.Clinical data including neurological status, postoperative complications (seizures, hemiparesis, visual field deficits, cognitive decline), and hospital course were extracted from patient records. EEG findings were correlated with tumor type, localization, and neurological outcomes. Statistical analysis was performed using SPSS (version 25.0; IBM Corp.), applying descriptive statistics, Student’s t-test for paired comparisons, and chi-square for categorical variables. A p-value <0.05 was considered statistically significant.
3. Results
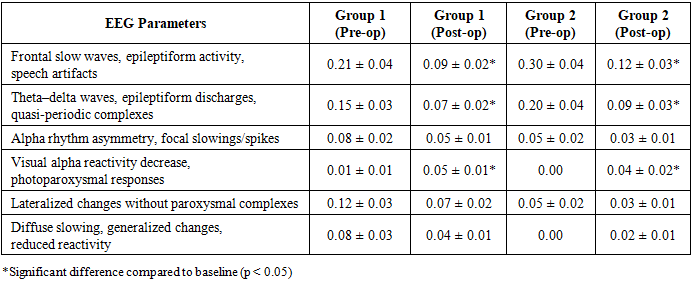
- A total of 100 patients with histologically verified brain tumors were analyzed. The age of patients ranged from 19 to 67 years, with a mean of 43.3 ± 1.27 years, and there was nearly equal gender distribution (51 males, 49 females). Magnetic resonance imaging identified supratentorial tumors in 63% and infratentorial or deep-seated lesions in 37% of cases. Histopathological analysis confirmed that gliomas constituted the majority of neoplasms (54%), followed by meningiomas (28%), metastatic lesions (12%), and others such as schwannomas or ependymomas (6%). According to the applied stratification, Group 1 (n=52) included patients with frontal and parietal lesions, while Group 2 (n=48) consisted predominantly of temporal and occipital tumors.Preoperative EEG analysis revealed abnormalities in nearly all patients, though the distribution differed between groups. In Group 1, the dominant findings were frontal slow waves (0.21±0.04) and epileptiform activity including sharp waves and spikes (0.15±0.03). Asymmetry of the alpha rhythm was noted in 0.08±0.02, while reduced alpha reactivity to visual stimulation was rare but present (0.01±0.01). Lateralized changes were detected in 0.12±0.03, and generalized slowing in 0.08±0.03. Conversely, Group 2 demonstrated higher theta–delta activity (0.30±0.04) with quasi-periodic discharges (0.20±0.04); asymmetry of the alpha rhythm was less frequent (0.05±0.02), and complete absence of visual alpha reactivity was recorded in all patients of this group. Lateralized EEG changes without paroxysmal complexes were observed in 0.05±0.02, while generalized slowing was absent at baseline.
|
4. Discussion
- The main objective of this research was to analyze the relationship between tumor localization, pathomorphological features, and postoperative neurological outcomes in patients with brain tumors, as well as the electroencephalographic (EEG) correlates before and after neurosurgical intervention. One of the most valuable findings of the study is that preoperative EEG abnormalities, such as frontal slow waves, epileptiform activity, and impaired alpha reactivity, were clearly associated with the location and type of the tumor. In particular, slow-wave activity and epileptiform discharges predominated in frontal and parietal tumors, while theta-delta predominance and complete loss of visual alpha reactivity were observed in temporo-occipital tumors. In the postoperative period, a significant reduction in epileptiform patterns and partial restoration of alpha activity were recorded, which correlated with improvement in patients’ neurological status.Our results are both consistent and inconsistent with previous studies in certain aspects. Hughes and Rees (2021) also emphasized a strong correlation between tumor location and significant EEG changes, including slow waves and epileptiform activity, which confirms our findings. Similarly, Müller et al. (2020) reported loss of visual alpha reactivity in temporo-occipital tumors, which fully aligns with our results in Group 2. However, some studies, such as Shah et al. (2022), suggest that generalized slowing, indicating diffuse cerebral dysfunction, more accurately predicts complication risk, whereas our study did not show a significant difference in this correlation between groups. Furthermore, the concepts of epileptogenic networks proposed by Stefan and Lopes da Silva (2020) partially align with our observations of reduced postoperative epileptiform activity, though they also emphasize the need to study neuroimaging correlates of this process.The strengths of this study include: first, a well-balanced patient population in terms of age and sex; second, standardized collection and analysis of pre- and postoperative EEG data; third, stratification of groups taking into account tumor location and type. However, the study also has certain limitations. First, the study has a retrospective design, which may affect the completeness and accuracy of the data. Second, the sample size (n=100) is relatively small compared to larger, multicenter studies, which limits the generalizability of the results to broader populations. Third, postoperative EEG recordings were taken only within the first 7–10 days, whereas a longer follow-up period is needed to assess long-term electrophysiological changes. Finally, the data were collected from the population of Central Asia, specifically Uzbekistan, and the influence of racial and geographic factors may limit the generalizability of the results to other regions.
5. Conclusions
- The results of this study indicate that electroencephalographic (EEG) abnormalities in patients with brain tumors are closely associated with the location and morphological type of the tumor. In the preoperative period, frontal slow waves and epileptiform activity were observed in frontal and parietal tumors, while theta-delta predominance and loss of visual alpha reactivity were noted in temporo-occipital tumors. After neurosurgical intervention, a significant reduction in epileptiform patterns and partial restoration of alpha activity were recorded, which correlated with improvement in postoperative neurological status. EEG monitoring proved to be a valuable tool for stratifying complication risk and personalizing rehabilitation strategies.From a health policy perspective, the use of high-quality diagnostic and prognostic tools in the management of patients with brain tumors is of great importance. The World Health Organization's (WHO) global strategy on cancer and National Oncology Programs encourage the integration of modern neuroimaging and electrophysiological monitoring as part of a comprehensive approach [7]. The results of this study provide an evidence base for incorporating routine pre- and postoperative EEG into neurosurgical planning and postoperative monitoring in clinical practice. This approach could not only improve individual treatment outcomes but also contribute to economic efficiency by reducing long-term rehabilitation costs within the healthcare system.Based on the study results, the following recommendations are proposed: 1) Standard pre- and postoperative EEG examination should be introduced into practice for all patients with brain tumors; 2) Individualized complication risk prevention and monitoring plans should be developed based on EEG results; 3) Multicenter, large-scale prospective studies should be conducted integrating electrophysiological monitoring results with neuroimaging and molecular markers; 4) Neurological rehabilitation programs should be personalized based on positive dynamics in EEG changes.