-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 489-494
doi:10.5923/j.ajmms.20261602.23
Received: Jan. 2, 2026; Accepted: Jan. 26, 2026; Published: Feb. 3, 2026

The Role of GSTM1 Gene Polymorphism in the Development of Bronchiectasis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhamidova F. M., Norjigitov A. M.
Department of Pathological Anatomy, Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents a comprehensive analysis of a retrospective, diagnostic study of bronchiectasis in the population of the Samarkand region. The inclusion and exclusion criteria of patients were carefully studied, confirming the validity of the selected study groups. Particular attention is paid to the comparative histological and genetic analysis of patients with bronchiectasis. Bronchiectasis is more common in the city of Samarkand, Urgut and Narpay districts. The disease is seasonal, reaching its peak in the spring and autumn seasons. For the study, the results of pathomorphological - general histological, histochemical and morphometric examination of bronchi and lung lobes of 48 patients who underwent lobectomy due to bronchiectasis, as well as the results of laboratory biopsies (blood) of 50 patients with bronchiectasis to study the (dell) mutation of the GSTM1 gene polymorphism were studied.
Keywords: Bronchiectasis, GSTM1, Morphometry, Patomorfology
Cite this paper: Khamidova F. M., Norjigitov A. M., The Role of GSTM1 Gene Polymorphism in the Development of Bronchiectasis, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 489-494. doi: 10.5923/j.ajmms.20261602.23.
1. Introduction
- Bronchiectasis is a chronic acquired and, in some cases, congenital disease characterized by irreversible changes (dilation, deformation) of the bronchi, accompanied by their functional impairment, impaired drainage function and chronic purulent-inflammatory processes in the bronchial tree, peribronchial space, the development of atelectasis, emphysema and cirrhosis of the lung parenchyma [1].Respiratory system diseases occupy a leading position among all diseases. The same trend is observed in pediatric practice, where their share is more than 70% [2]. Studies have shown that the prevalence of bronchiectasis detected by computed tomography (CT) in patients with COPD varies from 4% to 72%, depending on the bronchiectasis criteria and the populations studied. In contrast, approximately 20% of cases of COPD are recorded as the primary diagnosis in US and European bronchiectasis registries [3].Genetic defects can also play a role in the development of bronchiectasis. In modern pulmonology, chronic nonspecific lung diseases are considered multifactorial, based on the increased sensitivity of the body to environmental factors. The genetic component, mainly single nucleotide polymorphisms (SNPs), plays an important role in their manifestation. Polymorphisms affecting the semantic parts of genes often lead to the exchange of amino acids and the emergence of proteins with new functional properties [4].GSTT1 (Glutathione S-transferase theta 1) is a phase II detoxification gene (22q11.23), encoding an enzyme that ensures the binding of glutathione to toxic metabolites and protects cells from oxidative stress. The GSTT1 (0) deletion polymorphism leads to the loss of enzymatic activity and is associated with increased inflammation and adverse disease outcomes, while the functional allele is protective, including in pneumonia in children.A number of studies have shown that genetic polymorphisms in genes encoding enzymes responsible for the biotransformation of xenobiotics contribute to the development of bronchopulmonary diseases such as chronic obstructive pulmonary disease (COPD) [5]. Carriers of the dell haplotype of GSTT1 and GSTM1 have an increased risk of developing COPD [6]. However, a number of authors have not identified such associations [7,8].Recently, there is increasing evidence that single nucleotide polymorphisms play an important role in the development of immune responses by shaping certain gene alleles. Genetic predisposition may include specific polymorphisms that determine the level of antioxidant protection. It can increase the risk of developing diseases at any stage: both during pregnancy and after childbirth.Many studies have shown that the risk of developing bronchopulmonary diseases with combined polymorphisms of different genes is higher than with a single gene defect. Homozygotes for the "dell" alleles of two genes at once, GSTM1 0/0 and GSTT1 0/0, are risk factors for the development of asthma. The accumulation of defects in the glutathione-S-transferase family system contributes to the persistent, severe course of asthma in children. In asthma, genetically determined defects in the production of xenobiotic detoxification enzymes GSTT1 and GSTM1, which occur as part of limited allergic damage to the airways in children without a family history of allergic heredity, have been shown to be a leading link in the pathogenesis of the disease [9].A meta-analysis of 12 studies (4484 participants) showed that GSTM1-dell and GSTT1-dell genotypes significantly increased the risk of oral submucosal fibrosis. The associations were strengthened by the large sample size and high exposure to areca nut. The results support the role of GST polymorphisms in the pathogenesis of the disease and their importance in risk stratification and early diagnosis [10].A significant relationship was found between the child's age and the consumption of seafood and canned fish, legumes, cereals and starchy foods with the level of mercury in the blood (p<0.05). A significant interaction was found between the consumption of canned fish and the GSTP1 gene polymorphism: increased mercury levels were observed only in children with the Ile/Ile and Ile/Val genotypes. The data obtained require confirmation in other populations [11].The study was aimed at assessing the influence of environmental factors and polymorphisms of the glutathione-S-transferase (GSTT1, GSTM1, GSTP1) genes on the likelihood of detecting elevated blood aluminum concentrations in children. The sample included 366 children aged 2-8 years with typical development (control group, Jamaica). Consumption of legumes was associated with a higher likelihood of detecting aluminum in the blood, while a higher level of parental education reduced this risk. A significant interaction was found between seafood consumption and GSTP1 genotype: the likelihood of detecting aluminum was observed only in children with the GSTP1 Ile/Ile genotype. The results obtained require confirmation in other populations [12].Therefore, one of the urgent problems in our study is the study of GSTM1 gene polymorphism in patients with bronchiectasis in the Samarkand region using pathomorphological and molecular genetic methods.Research Aim. The aim of the study is to study the GSTM1 gene polymorphism (dell) mutation in patients with bronchiectasis in the Samarkand region using pathomorphological and molecular genetic methods.
2. Materials and Methods of Research
- The study examined the results of pathomorphological - general histological, histochemical and morphometric examination of bronchi and lung lobes in patients who underwent lobectomy due to bronchiectasis, as well as laboratory results of biopsy (blood) from patients with bronchiectasis to study the polymorphism (dell) mutation of the GSTM1 gene.For this, the patients in our study were divided into 3 observation groups.Group 1 was a control group, which included 12 cases of bronchial and lung biopsy specimens from patients who died of respiratory diseases, and 20 cases of biopsy specimens (blood) from healthy individuals who did not have bronchiectasis to detect the GSTM1 gene polymorphism (dell) mutation.In 2 groups - 34 cases were included, in which patients who underwent lobectomy due to bronchiectasis were treated with biopsies of bronchus and lung lobes.In group 3, blood from 30 patients was used to study the GSTM1 gene polymorphism (dell) mutation in patients with bronchiectasis.Inclusion criteria: To be included in the study, patients with bronchiectasis must be over 18 years of age, have a diagnosis of bronchiectasis confirmed by radiology and high-resolution computed tomography, and have clinical symptoms consistent with bronchiectasis (cough, sputum production, shortness of breath, or respiratory infections) with a clinical diagnosis of J 47 on the ICU.Exclusion criteria: Patients were excluded from the study if they were unable to provide informed consent or if they had active tuberculosis or lung cancer. Patients with cystic fibrosis or pulmonary fibrosis with secondary bronchiectasis were also excluded.Patients in the bronchiectasis groups were required to be clinically stable and not taking antibiotics or oral corticosteroids for 4 weeks prior to study entry. All relevant medical history (comorbidities, current medications, significant past illnesses, surgeries, and diagnostic procedures) was recorded at screening.Bronchiectasis was defined as bronchial dilatation on high-resolution CT, clinical signs, airway obstruction, and a history of smoking. To be included in the “bronchiectasis” cohort, participants had to have a CT scan within the past 5 years that showed evidence of bronchiectasis. In addition, to be included in the bronchiectasis cohort, participants had to have no clinical diagnosis of COPD and no relevant smoking history (<10 pack-years) and/or no airway obstruction as determined by spirometry at screening.
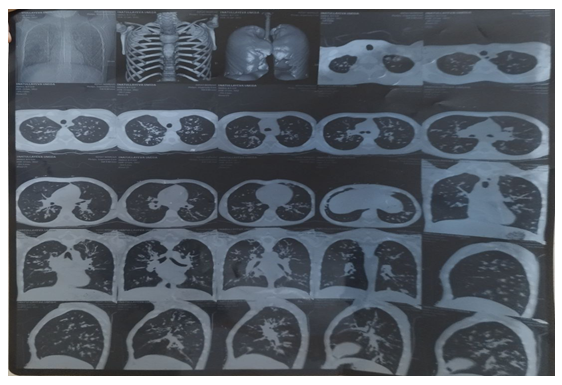 | Figure 1. Patient I.U. is 24 years old. According to the results of high-resolution computed tomography (CT) of the chest, diffuse changes in the bronchial tree are detected in both lungs. In some segmental and subsegmental bronchi, their diameter is larger than the diameter of the adjacent pulmonary arteries. Thickening of the bronchial walls and their clear visualization up to the peripheral sections are noted. |
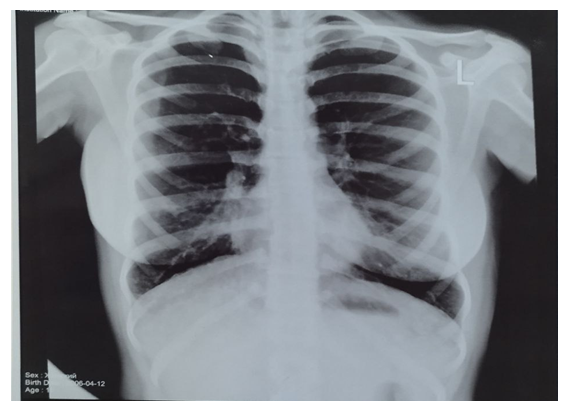 | Figure 2. Patient M.M. is 30 years old. The radiograph shows increased lung volume and deformation in both lung fields, mainly in the lower sections. The coarse and uneven appearance of the bronchovascular pattern indicates a chronic inflammatory process in the bronchial walls |
3. Research Results
- When comparing cohorts of patients in all observation groups, bronchiectasis was more common in women, in 11 cases (66.33%), and in men, in 19 cases (36.66%) (Fig. 3).
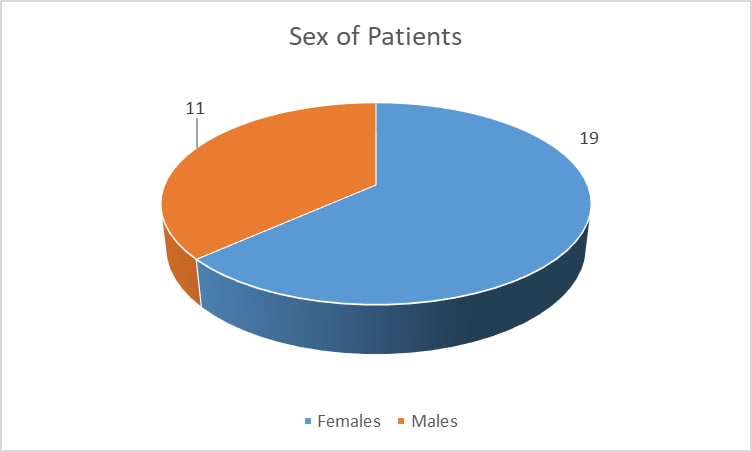 | Figure 3. Sex-related incidence of bronchiectasis in a follow-up group |
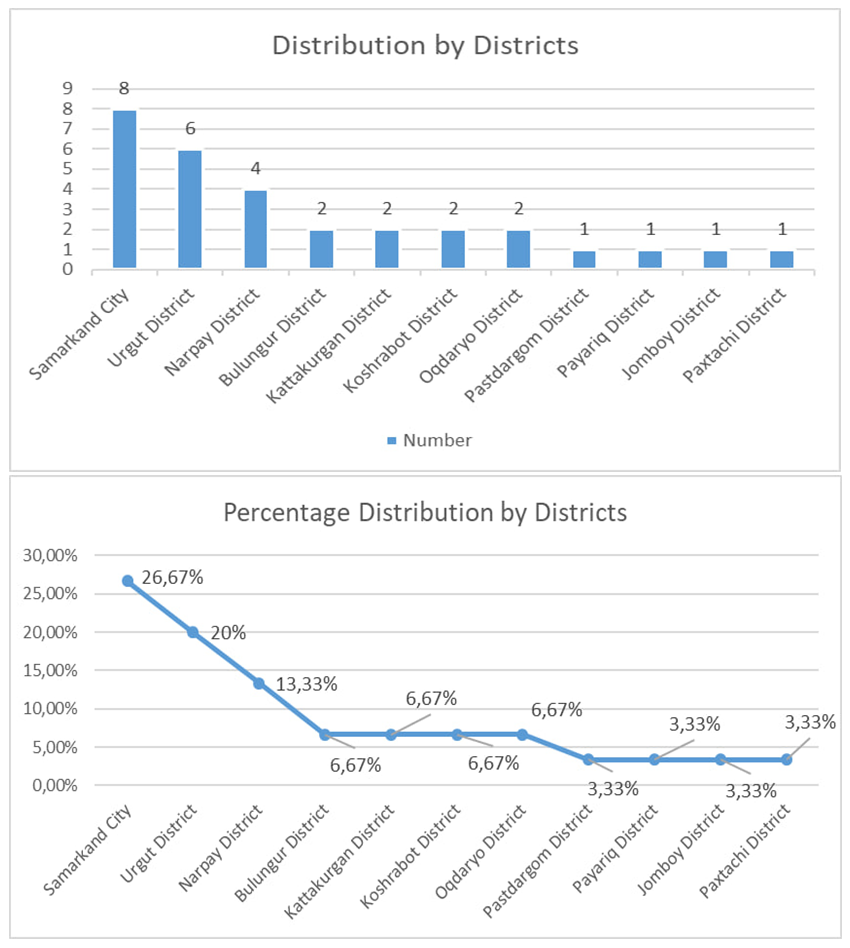 | Figure 4. District-level incidence of bronchiectasis in Samarkand region |
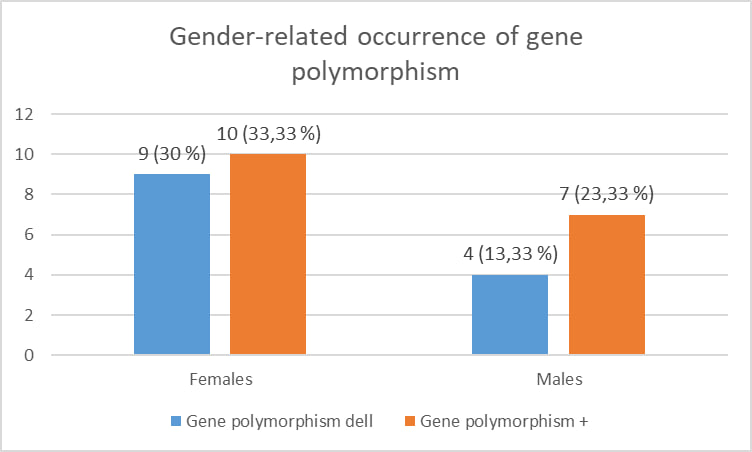 | Figure 5. Gender-related occurrence of gene polymorphism |
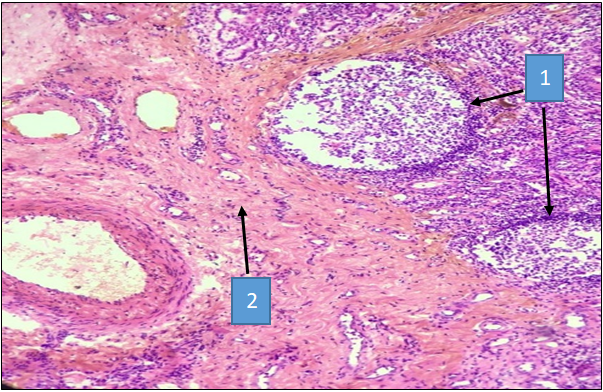 | Figure 6. Bronchiectasis. Lung tissue of a 48-year-old patient. The lung tissue shows large focal lymphocytic infiltration (1), areas of destruction and sclerosis (2). Hematoxylin and eosin staining. Cat. X40 |
 | Figure 7. Bronchiectasis. Lung biopsy of a 52-year-old patient. Sclerosis (1) and vascularization (2). Hematoxylin and eosin staining. Cat. X40 |
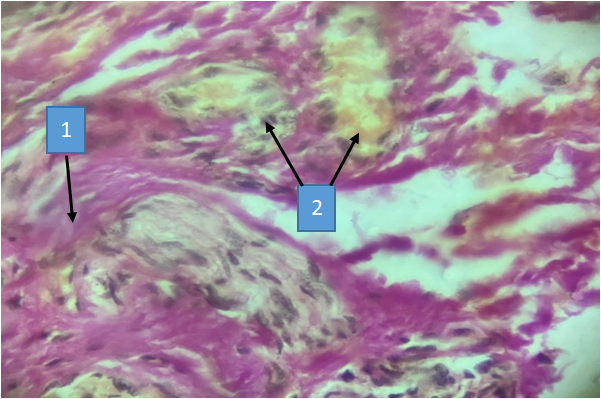
 | Figure 8. Bronchiectasis disease. A 47-year-old patient with a small-caliber bronchus fragment. Serous glands in the bronchi are hypertrophied (1), in a state of hypersecretion (2), and most of them show accumulation of secretion and destruction (3). Staining according to Van-Gieson |
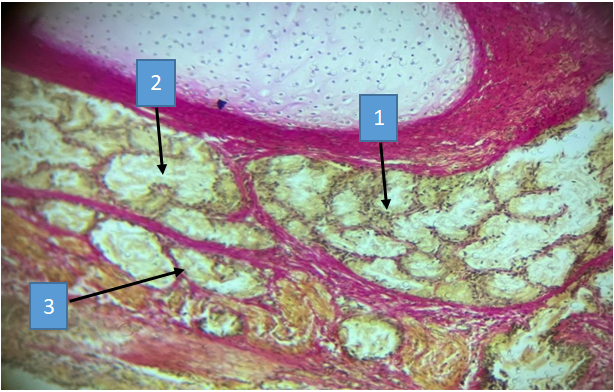
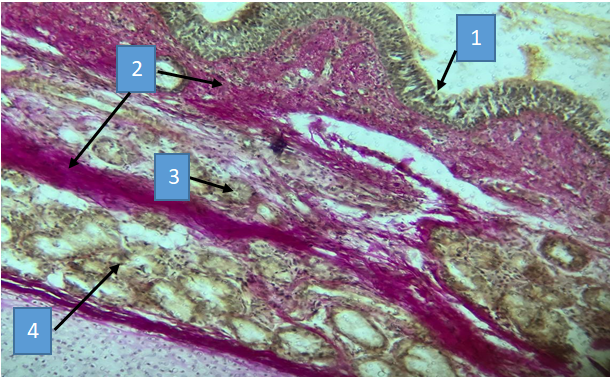 | Figure 9. Bronchiectasis disease. A 47-year-old patient with a small-caliber bronchus fragment. Hyperplasia of the bronchial mucosa (1), sclerosis of connective tissue and muscle fibers of the submucosa (2), destruction and necrosis of serous and protein glands (3), hypersecretion (4). Staining according to Van-Gieson. Cat. X40 |
4. Conclusions
- Bronchiectasis is more common in the city of Samarkand, Urgut and Narpay districts. The disease is seasonal, reaching its peak in the spring and autumn seasons.For the study, the results of pathomorphological - general histological, histochemical and morphometric examination of bronchi and lung lobes of 48 patients who underwent lobectomy due to bronchiectasis, as well as the results of laboratory biopsies (blood) of 50 patients with bronchiectasis to study the (dell) mutation of the GSTM1 gene polymorphism were studied.