-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2026; 16(2): 426-429
doi:10.5923/j.ajmms.20261602.08
Received: Jan. 7, 2026; Accepted: Jan. 27, 2026; Published: Feb. 3, 2026

Advanced Treatment Strategies for Removable Denture-Induced Oral
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRasulova Mokhigul Matyokub kizi
Assistant, Department of Anatomy, Clinical Anatomy (OSTA), Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Rasulova Mokhigul Matyokub kizi, Assistant, Department of Anatomy, Clinical Anatomy (OSTA), Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Removable denture prostheses are one of the major etiological factors contributing to oral mucosal lesions, including prosthetic stomatitis. Mechanical trauma, microflora imbalance, and impaired local immunity play a key role in the development and persistence of inflammatory changes. In denture wearers, mucosal pathology tends to progress gradually, often presenting with subtle clinical signs that complicate early diagnosis and timely therapeutic intervention. Recent research has focused on optimizing treatment strategies aimed at accelerating epithelial regeneration, normalizing local pH, reducing hyperemia and discomfort, as well as improving patient compliance. Comparative studies indicate that modern therapeutic approaches may demonstrate better clinical efficacy than conventional methods. The identification of reliable, non-invasive clinical markers of inflammation can contribute to earlier detection and improve treatment outcomes in patients with removable denture-induced oral mucosal lesions.
Keywords: Removable dentures, Oral mucosa, Prosthetic stomatitis, Epithelial regeneration, Hyperemia, pH, Modern therapy
Cite this paper: Rasulova Mokhigul Matyokub kizi, Advanced Treatment Strategies for Removable Denture-Induced Oral, American Journal of Medicine and Medical Sciences, Vol. 16 No. 2, 2026, pp. 426-429. doi: 10.5923/j.ajmms.20261602.08.
1. Introduction
- The oral mucosa is a complex biological structure that exhibits several unique physiological characteristics. Its protective potential is largely attributed to its capacity to withstand numerous types of harmful influences, including mechanical trauma, chemical irritants, fluctuations in temperature, and the continuous action of microbial and toxic metabolic products. One of the most distinctive features of the oral mucosa is its remarkable regenerative ability, which ensures rapid cell turnover and restoration of tissue integrity following injury [2]. Nevertheless, despite its robust defensive capacity and specialized biological functions, diseases affecting the oral mucosa remain highly prevalent and constitute one of the most challenging and clinically significant problems in dentistry.Epidemiological data from the World Health Organization indicate that more than 90% of the middle-aged and elderly population suffer from disorders of the oral mucosa and periodontal tissues [1]. The high incidence of such conditions can be attributed to a combination of local and systemic factors including aging, chronic somatic diseases, metabolic syndrome, long-term medication use, immune dysregulation, and the widespread application of removable prosthetic appliances. These elements collectively impair mucosal homeostasis, weaken protective mechanisms, and promote the progression of inflammatory and degenerative lesions.According to A. E. Zarkumova, the insufficient therapeutic effectiveness of current treatment modalities and the broad impact of adverse environmental factors on the dentoalveolar system as well as on the human body necessitate a more detailed classification of inflammatory mucosal disorders [4]. This reflects a major scientific and practical challenge for contemporary dentistry and underscores the need for innovative approaches aimed at improving diagnostic accuracy, preventive strategies, and treatment outcomes.A growing number of studies support the view that pathological processes observed in the oral cavity are closely associated with systemic diseases, including endocrine disorders, gastrointestinal dysfunction, metabolic abnormalities, and deviations in immune status. The variety of dental problems, their multifactorial etiology, and the similarity of clinical manifestations across different nosological forms further complicate the task of diagnosis and require evidence-based therapeutic guidelines [3]. From a clinical standpoint, the interconnection between oral and systemic health has stimulated considerable interest in the development of non-invasive diagnostic markers and new disease models aimed at early detection and more precise risk stratification.Saliva, in particular, has emerged as a promising biomarker source and a valuable tool for the diagnosis and monitoring of oral mucosal diseases. It is an easily obtainable biological fluid that contains a wide range of protective molecules, including antimicrobial peptides, immunoglobulins, enzymes, antioxidants, growth factors, and cytokines. These components play an essential role in maintaining oral homeostasis and providing first-line defense against pathogens. Comprehensive investigation of salivary biomarkers offers new possibilities for enhancing early diagnosis, differentiating similar pathological conditions, and monitoring treatment responses in clinical practice [5].Removable denture prostheses represent one of the most significant etiological factors contributing to injuries and inflammatory conditions of the oral mucosa in elderly individuals. Denture-related changes are often multifactorial in origin, involving mechanical irritation, microbial dysbiosis, local immune suppression, and biochemical alterations in the denture-bearing tissues. Several authors have demonstrated that prosthetic appliances can alter the acid–base balance and mineral composition of mixed saliva, potentially influencing oral microbial ecology and favoring the development of pathological processes [6].
2. Materials and Methods
- The study was carried out at the Department of Orthopedic Dentistry and the Stomatology Center of the Bukhara State Medical Institute named after Abu Ali ibn Sina. A total of 149 patients (Table 1) requiring removable denture prosthetic treatment were examined during the study period (2024–2025). Depending on the clinical condition of the oral mucosa and the applied therapeutic approach, the patients were divided into three groups: a control group, a conventional therapy group and a modern therapy group.
|

3. Results
- Prior to treatment, the majority of patients exhibited pronounced inflammatory signs in the oral mucosa. Among subjective complaints, pain, itching, and burning sensations were predominant, with an average intensity of 6.8 ± 1.2 points on the Visual Analog Scale (VAS). Clinical examination revealed diffuse erythema, edema, and, in some cases, areas of erosion on the mucosal surface, with the overall frequency of inflammatory signs reaching 100%.The study results indicated that patients rehabilitated with partial removable dentures demonstrated significant positive changes in the condition of the oral mucosa following treatment with Calendula officinalis (Calendula officinalis extract) extract (Table 2). Prior to therapy, mucosal hyperemia was observed in 100% of patients, swelling in 100%, and erosion or ulceration in 38%. The average sub-denture reactivity score was 2.8 ± 0.4, the Oral Hygiene Index–Simplified (OHI-S) was 4.5 ± 0.6, pain intensity on the VAS scale was 6.7 ± 1.1, and denture adaptation was 0%.
|
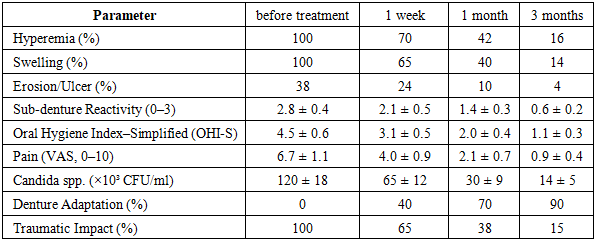
4. Conclusions
- Overall, these results demonstrate a clear trend of progressive improvement in oral mucosal health during denture treatment. The reduction in hyperemia, swelling, and erosive lesions, along with decreased subprosthetic reactivity and pain scores, highlights the effectiveness of the applied treatment protocol. Furthermore, the improvement in denture adaptation underscores the importance of both proper prosthetic design and patient education in achieving optimal functional and clinical outcomes. This progressive recovery process also emphasizes the critical role of continuous oral hygiene monitoring and management in patients receiving removable prostheses.Treatment with Calendula officinalis extract significantly reduced pain and mucosal inflammation in patients with prosthetic stomatitis. Clinical observations showed that in 78% of patients, pain levels decreased to 0–3 points on the Visual Analog Scale (VAS), confirming the extract’s effectiveness in alleviating dental discomfort. Patients treated with Calendula officinalis extract extract demonstrated a marked reduction in mucosal hyperemia and erosive changes within 14 days. Clinical follow-up confirmed that 85% of patients achieved complete mucosal regeneration with the absence of inflammatory signs. Microbiological analysis revealed that treatment with Calendula officinalis extract significantly reduced pathogenic oral microflora. The levels of Streptococcus mutans and Candida albicans decreased on average by 2.5–3 times, indicating the extract’s antimicrobial efficacy in both the prevention and management of prosthetic stomatitis. with Calendula officinalis extract extract also enhanced patient tolerance to removable dentures. During the study, 90% of patients reported a substantial reduction in discomfort and pain while wearing dentures, supporting the use of the extract as an effective adjunct in prosthetic rehabilitation.